Background:
The electrical injuries are a specific type of thermal trauma which depends pathophysiologically on the electrical voltage and the resistance of the tissues. The transition of the electricity through the body is unpredictable, but generally it starts from an entry point and moves on to a grounded object (15). The resistance of the tissues in the contact area of the human body affected by electricity is crucial about the severity of the injury. When passing through the body the electricity converts into heat (21, 9). The extent of damage of tissues depends on the intensity and the continuance of the heating (9). Electricity generates more heat in less conductive tissues. The gradation of tissues from most conductive to least conductive is as follows: neural tissue, blood vessels, muscles, skin, adipose tissue, bones (15).
Materials and methods:
We are presenting a case of a 32-year-old man registered in the emergency room at Plastic, Recovery and Aesthetic Surgery Clinic at “St. George Hospital” Plovdiv. Case history – high voltage electric cable contact; subjectively: sensation of pain in contact area – the right arm and the head; objectively: general condition – injured, involuntary left-sided position, conscious, contact, adequate, good orientation, stable hemodynamics. ECG – sinus rhythm. While observing the local status we found an 8 % area of third degree burns with an intense edema and a flexion contracture on the elbow joint of the right upper limb, third degree burns with parietal-occipitally located dense dry necrosis covering an area of 170 sq. cm. (11/16 cm.) on the head. The burn on the lower limbs, where supposedly is the exit orifice of the electricity, are of IIAB-III degree with well-formed deep necroses on the IV-th and the V-th toes of the right foot and on the I-st and the II-nd toes and the back of the left foot. The laboratory parameters correspond to the underlying disease (haemoconcentracion, hypoproteinaemia, hypoalbuminaemia, high levels of transaminases). The patient was treated surgically urgently, necrotomia and fasciotomia of the right hand. On the third day after the accident the right upper limb was amputated at the level of medium-upper third humerus, and later on re-amputated at the level of proximal third right humerus on the right. The patient underwent a stepwise debridement in the area of the toes of both feet and the back of the left foot as well as a covering of the tissue defect by using local tissues and a free skin autologous transplant. During hospital admission (1,9 hours after the trauma) in consultation with neurosurgeon and after a CT-scan of the cranial fossa and the cerebrum we did not detect lesions or some data for minimal residual disease (MRD)and neurologycal symptoms of . On the 9-th day after the trauma because of reduced mobility of both lower limbs we recommended a re-consultation with a neurologist which resulted in the following conclusions: MRD (-) ; cranial nerves (-) hypoesthesia Th 4-5 (left) and Th 8-9 (right) .
On the 17-th day after the trauma we observed a progressive quadriplegic syndrome. We recommended a control CT-scan of the head, the cervical, the thoracic and the lumbar areas of the spinal cord, but the results did not show neither any lytic changes nor any damages of the calvaria. The conclusion of the neurosurgeon was Electro-myelopathy with quadraparesis. We surgically removed the soft-tissue necrosis in the parietal-occipital area. We found out a necrotic osteomyelitis of the underlying calvaria with subsequent osteodebridement, purulent malodorous collection over durra mater covered with surface necroses and a total thrombosis on the front sagital sinus. In-depth we found nothing, no leaks of purulence or cerebrospinal fluid. Subsequent revision, debridement, lavage. The tissue defect formation was covered in two stages with two bridge-flaps (occipital and frontal) by using combined techniques and the donor areas and partially the primary defect were covered by using a free skin plasty. Postoperative CT-scan results: wide parietal-occipital trepanation with 11 cm. diameter of the defect, no data for lesions or inflammatory changes in the brain structures or maters. The postoperative period ran smoothly. The plegic syndrome reversed in a 5-days period. The patient was discharged from the hospital on the 8-th day after the last operation in much better condition.
Discussion:
The electric burns in the scalp area represent 3% of all electric traumas and 1% of all other burns (15, 6). However there are some single cases of high-voltage burns affecting brain structures described in the professional literature. The difference in conductivity is the reason for the significant changes of the deeper located tissues caused by thermal injuries as compared to the considerably less damages of the skin. In cases of electrical traumas the damages of the bones and the deeper located structure always exceed these of the skin. Norma (15) accepts that it is a specific feature of the cranial bones to dissipate heat slower than the other tissues and even after the termination of the effect of the source they continue heating up the neighboring tissues. In his studies Norma (15) writes that in cases of electric traumas recovery surgery is usually done 22 ± 6 days after the burn. Yet Buonanno (3) and Drrstelmann (7) opine that the best results can be achieved only providing early diagnosis and timely adequate treatment.
In the case we are presenting we performed surgery on the head area on the 37-th day after the trauma. There was some delay as compared to the cases described by other authors, due to the lack of pathological symptoms or lesions of the brain tissue and the severe damages on the right arm. According to Thron (23) the main obstacle to the early diagnosis of sagital sinus thrombosis are the non-specific primary symptoms (severe headache, nausea and vomiting), which rarely guide clinicians to such a disease. There may be other clinical signs such as focal neurological symptoms, symptoms related to III, IV and VI cranial nerves, vision loss, seizures and changes in psychological condition, but they may be hardly noticeable. Gurpreet (9) points out that the lack of neurological complications right after an electric trauma does not necessarily imply that some neurological sequelae will not occur later on. He believes that neurological sequelae may occur even three years after the trauma. Levine (14) and Breugem (2) describe several cases of quadriplegia caused by high-voltage electric injuries, where the neurological symptoms occurred several days or even weeks after the injuries and are slowly progressing. In our case the reduced mobility of the limbs occurred on the 9-th day and gradually became a quadriplegia.
According to Thaventhiran (22) patients show different recovery rates for a period of several weeks to 5 years after the trauma. In our case there was a quick reverse of the quadriplegic syndrome shortly after the surgery and there were residual paretic symptoms for two years after the trauma.
The pathophysiological changes of the delayed neurological impairment is still a matter of discussions. Cooper (5) believes that the progressive micro-vascular occlusion may lead to ischemia and intra neural thrombosis. Christensen (4) associates the impairment with a change of the intracellular DNA and some enzymes (injuries depending on the type of the irradiation), which lead to disruption of cell division and death of nervous tissue.
Some other authors (10, 5, 13) point out that the electro-conformational changes in the membrane proteins may be the reason for the pore formation in cell membrane, which compromises the integrity of the cell wall and the cell functioning. On the other hand Lee (13) thinks that the reason for the delayed neurological impairment may also be the magnetic effect on tissues.
However none of these theories corresponds to the recovery period of our patient, who improved significantly in several days. Our experience showed us that the conventional X-ray of the skull had no informational value. There were no conventional X-ray graphic signs. Most authors believe that angiography is the best diagnostic method and should not be delayed if there is some clinical suspicion of thrombosis. The nuclear-magnetic resonance imaging is also a method, and some indirect computer-tomographic signs (venous heart attacks) are observed in all the patient with focal neurological symptoms, but they are rather delayed in time. In our case the repeated CT-scans of the cerebrum and the spinal cord did not show pathological lesions or thrombotic changes.
Various approaches are described and used for treatment of high-voltage electrical burns of the head, including partial or complete removal of the necrotic soft tissues and bones, subsequent allograft coverage and the delayed or the instant autografting (6,17,10,1,16,20).
Flaps from local tissues, as well as micro-vascular free flaps may be used for instant coverage. Hartford (10) insists that a partial debridement of bones is possible during the early phases, if afterwards the defect is covered by well-vascularized tissues. In this case the objective is preserving the contour of the skull by leaving a grate (made of many borated holes), which serves as a platform for bone regeneration with no additional cranioplasty necessary.
Nevertheless, other authors (8, 19) report about subsequent sequestration of bones and the necessity of secondary removal of the necrotic bones in cases of partial debridement of the affected bone segments.
We rather agree with Delay, Roelhl and Hartford (6, 17, 10), who think that boration and coverage with well-vascularized tissue is possible if the entire thickness of the bone is not affected. We postulated that the total osteo-debridgement was the only solution. We accepted that the two-basic flaps we used are a reliable and affordable method of reconstruction, which provides an adequate supply of blood to the flaps themselves and a coverage of the underlying tissues with intact tissues. Many other authors endorse this opinion (12, 11, 18).
We find the delayed final result of the treatment very satisfying. Four years after the trauma the formed bridge-flaps and the free transplants are absolutely vital and the shape of the calvaria is preserved. The general condition of the patient is much improved, no residual symptoms. We consider the alopecia in the area of the free grafts as a disadvantage, but it can be planned and corrected.
Conclusions: The high-voltage electrical traumas may lead to a significant impairment of the central nervous system. The clinical variability and the low frequency of the thrombosis of the front sagital sinus make clinical researches extremely complicated. The prognosis and the treatment of such patients should be consistent with the potential for delayed neurological deteriorate, including severe deficiencies such as quadriplegia.
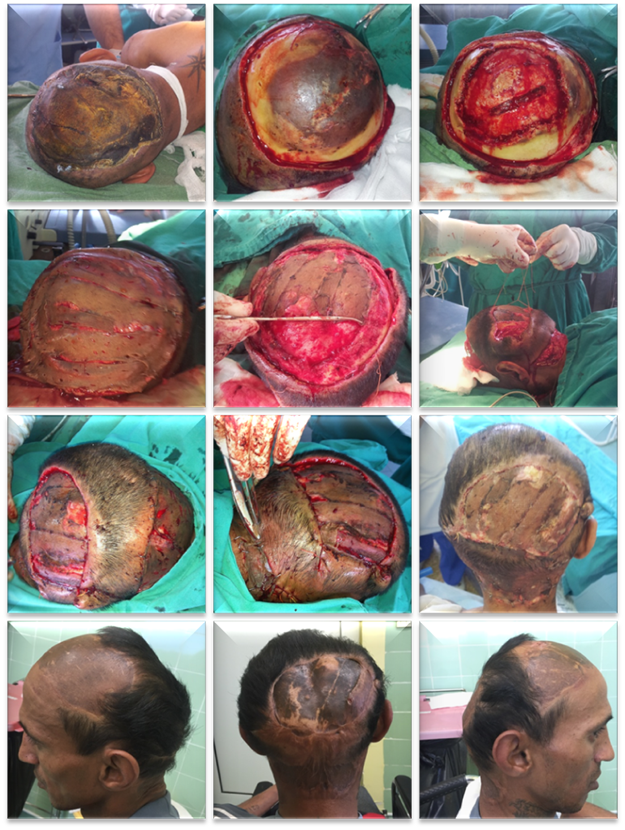
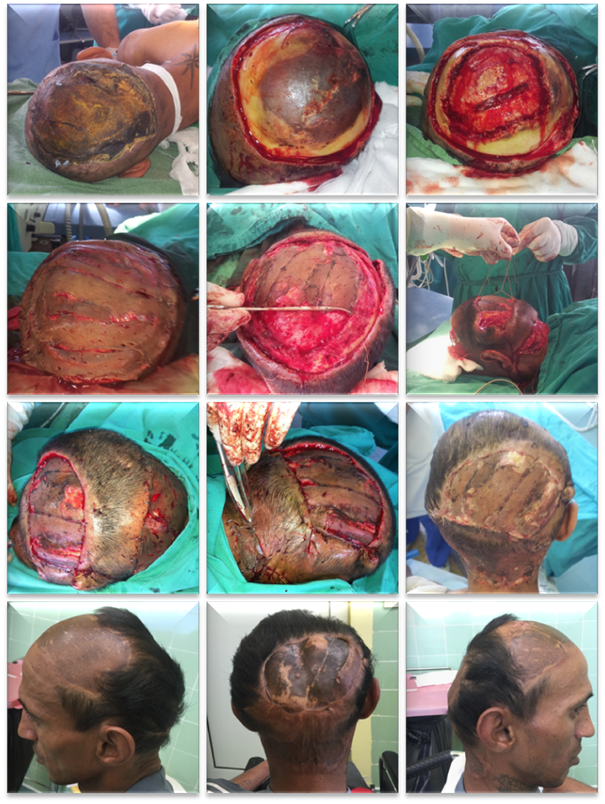
Fig 1. Stages of the surgical treatment and pictures 4 years after the surgery.
References:
- Bizhko IP, Slesarenko SV. Operative treatment of deep burns of the scalp
and skull. Burns 1992;18:220-223.
- Breugem C.C., Van H.W., Groenevelt F. High voltage electrical injury leading to a delayed onset tetraplegia, with recovery. Ann N Y Acad Sci, 888 (1999), pp. 131–136
- Buonanno FS, Moody DM, Ball MR, Laster DW (1978) Computed
cranial tomographic findings in cerebral sinovenous occlusion.
J Comput Assist Tomogr 2: 281-290
- Christensen J.A., Sherman R.T., Balis G.A., et al. Delayed neurologic injury secondary to high-voltage current, with recovery. J Trauma, 20 (1980), pp. 166–168
- Cooper M.A. Emergent care of lightning and electrical injuries. Semin Neurol, 15 (1995), pp. 268–278
- Dalay C, Kesiktas E, Yavuz M, Ozerdem G, Acarturk S. Coverage of scalp
defects following contact electrical burns to the head: A clinical series. Burns 2006;32:201-207.
- Drrstelmann D, Dobiasch H, Mattes W, Reuther R (1981) Hirnvenen-
und Sinusthrombose. Ein Beitrag zur Antikoagulantienbehandlung.
Nervenarzt 52 : 243-246
- Gumus N, Coban YK, Reyhan M. Cranial bone sequestration 3 years after
electrical burn. Burns 2006;32:780-782.
- Gurpreet Singh, Mohammad Kaif, Aman Deep, Peter Nakaji,
High-voltage electrical burn of the skull causing thrombosis of the superior sagittal sinus; Journal of Clinical Neuroscience; Volume 18, Issue 11, November 2011, Pages 1552–1554
- Hartford CE. Preservation of devitalized calvarium following high-voltage
electrical injury: case reports. J Trauma 1989;29:391-394.
- Jadhav CN , Kumar Sharma R .Bipedicled scalp flaps for reconstruction of high-tension electric burns of calvarium. J Craniofac Surg. 2014 Sep;25(5):e406-8.
- Karsidag S, Ozcan A, Ozkaya O, Ugurlu K, Bas L. Use of wide bipedicled pericranial flap in anterior scalp reconstruction. J Craniofac Surg. 2009 Nov;20(6):2248-51.
- Lee R.C, Gaylor D.C., Bhatt D., et al. Role of cell membrane rupture in the pathogenesis of electrical trauma. J Surg Res, 44 (1988), pp. 709–719
- Levine N.S., Atkins A., McKeel Jr. D.W., et al. Spinal cord injury following electrical accidents: case reports. J Trauma, 15 (1975), pp. 459–463
- Norma I. Cruz, Fanor M. Saavedra. Preservation of Nonviable Cranial Bone after Class IV Electrical Burns. PRHSJ Vol. 29 No. 1 • March, 2010
- Oishi SN, Luce EA. The difficult scalp and skull wound. Clin Plast Surg
1995;22:51-59.
- Roelhl K, Geoghegan J, Herndon DN, Patterson J, McCauley RL. Management of class IV skull burns using bipedicled superficial temporal artery
scalp flap. J Craniofac Surg 2008;19:970-975.
- Seok Ho Yoon, Jin Sik Burm, Won Yong Yang, Sang Yoon Kang Vascularized Bipedicled Pericranial Flaps for Reconstruction of Chronic Scalp Ulcer Occurring after Cranioplasty. Arch Plast Surg. 2013 Jul; 40(4): 341–347.
- Shen Z, Wang N, Ma C. Treatment of extensive deep burn of scalp with
full-thickness necrosis of calvarial bone. Zhonghua Zheng Xing Shao Shang Wai Ke Za Zhi 1995;11:10-12.u
- Spies M, McCauley R L, Mudge B P, Herndon DN. Management of Acute
Calvarial Burns in Children. J Trauma 2003;54:765-769.
- Stuckey J.G. The surgical management of massive electrical burns of the scalp. Plast Reconstr Surg, 32 (1963), pp. 538–543
- Thaventhiran J., O’Leary M.J., Coakley J.H., et al. Pathogenesis and recovery of tetraplegia after electrical injury. J Neurol Neurosurg Psychiatry, 71 (2001), pp. 535–537
- Thron A., Wessel K., Linden D., Schroth G., and Dichgans J.. Superior sagittal sinus thrombosis: neuroradiological evaluation and clinical findings.
J Neurol (1986) 233 : 283-288e[schema type=»book» name=»CASE REPORT OF HIGH VOLTAGE ELECTRICAL BURNS CAUSING SINUS SAGITALIS SUPERIOR THROMBOSIS» description=»Tissue defects in the head area, caused by high voltage electric burns and affecting the calvaria and the underlying brain tissues are a rare but very serious burn damage. Early diagnosis and adequate treatment are important prerequisites in prevention of severe complications. We are presenting a case of a 32-year-old man with a severe high voltage electric burn injury, a large parietal-occipital tissue defect, a deep necrosis reaching dura mater and a thrombosis of sinus sagitalis superior. The clinical symptoms are as follows – gradually progressing paresis causing a paraplegia of the lower limbs. A decompressing osteodebridgement of a large area of the calvaria resulted in a reversion of the lower paraplegia. Seeing the high risk of a mechanical trauma of the brain tissue we covered the tissue defect by a frontal and an occipital bridge-flap.» author=»Zanzov Elean, Anastasova Vania, Krasteva Elena» publisher=»БАСАРАНОВИЧ ЕКАТЕРИНА» pubdate=»2017-01-05″ edition=»ЕВРАЗИЙСКИЙ СОЮЗ УЧЕНЫХ_30.11.16_31″ ebook=»yes» ]