
Introduction
The treatment of burns and their consequences used to be a challenge since ancient times. Burns often lead to hypertrophic scars and deformations, which should be treated simultaneously with the main disease. The prophylaxis consists of atraumatic approach, proper treatment of fresh burns and post-operative prophylaxis. In the past functional deficiency was the basic reason for surgery. Nowadays the aesthetic result is of no less importance for the social adaptation of the patient.
Materials
For a period of eight years (2007-2014) in Department of Plastic, Reconstructive and Aesthetic Surgery at “St. George” University Hospital in Plovdiv we have performed 431 surgical interventions of patients with hypertrophic scars and contractures. 45 of them underwent more than one surgery. In most cases we undertook surgery approximately two years after the fresh burn. In cases of severe functional changes on the neck, major joints and face we undertook surgery right after their formation.
We divided our patients by demographic signs – sex and age.
Division by sex: men 248 (57,5%), women 183 (42,5%).
Division by age: adults (55%) and children (45%).
According to aetiology we analyzed the causes for the fresh burn. Here is the classification – flame burns, scald injuries, electrical, chemical and contact ones.
The defects are usually located in the following areas: head, neck, upper limb, body, axilla, lower limb. There is a separate class of surgical patients with more than one location.
Another division is the one based on the hospital stay – short duration (up to 5 days), medium duration (5-10 days) and long duration (over 10 days).
We analyzed the data of all our patients according to the used surgical technique as well. We practiced excision and direct closure, skin grafting, flaps, expander technique, lipofilling, dermabrasion and various combinations of these techniques. We present Z-pasty as a separate procedure of the PNL because of its frequent use. Besides we oversaw the contractures, keloids and syndactyly as burn consequences.We used the following clinical methods – case history and objective physical examination. Diagnostic methods – laboratory tests.
We processed the data of our research by using the spacial pack SPSS 16.0 (IBM Corporation, Armonk, NY). All average values are presented as results ± arithmetic mean error. The statistic criteria are considered valuable if p < 0.05. We processed the statistics by using frequency division analysis, alternative analysis, non-parametric analysis, dispersion analysis, correlation and regression analysis, graphic analysis.
Methods
We practiced excision and direct closure in patients with limited defects. We removed hypertrophic tissues by using scalpel and scisors. We indispensably removed the connective tissue fibers from each wound bed regardless of the used surgical technique afterwards. After undermining the we sutured without pressure.

Fig №1 Excision and direct closure
We practiced free skin plasty as a split-thickness skin graft (STSG) and a full-thickness skin graft (FTSG). As donors we used mainly the inguinal, retroauricular area and the supine surface of the brahium, followed by drainage perforations, fat tissue removal and stapler fixation on the anticipatory wound surface. This technique is used basicly on functional areas such as the face and the hands.

Fig. № 2 Full-thickness skin graft
Split-thickness skin graft are (STSG) used mainly in cases of extensive cicatricial changes. They are taken into electrodermatom, perforated and fixed. We applied a sterile ointment bandage with Bactigras in both types of transplants.

Fig. №3 Split-thickness skin graft
The flaps are the main surgical technique in our study. We used mainly local flaps (rotation, transposition, advancement) as well as transposition of triangle flaps (Z-plasty) with symmetric and non-symmetric figures. Pedicle flaps were formed as forearm flap, frontal flap, parascapular flap etc. We adhered the ratio length/width from 1:1 to 2:1 in well vascularised areas such as the upper limb and the face.
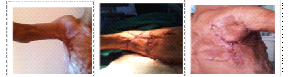
Fig. №4 PNL
We usually used Z-plasty in order to release contractures. In general section, mostly located on brides, we form general figure containing two or more opposite triangles. Thus the towing line of the scars is interrupted. More frequently we formed symmetric figures with equal side length and same angles. We use non-symmetric figures only in cases of insufficient skin resources on one of the sides. In such cases the sides are equal as well, but the angles are of different size.

Fig. №5 Z-plasty
We used expander technique in cases of post-burn alopecia, reconstruction of neck and face and deformations of limbs. We used square and crescent-shaped expanders. Filling the expander after the insertion takes about two months. In all cases we put 10% of the volume intaoperatively and then practiced hyperexpansion.

Fig.№6 Expander technique
This is a widely used combination of surgical methods, because the surrounding tissue is modified, the defect is wide and there is a necessity of several surgeries. The major combination is the one of flaps and skin grafting technique.
Results
The frequency of post-burn consequences is presented in the following table:
Table № 1 Division by frequency and year
Results by demographic sign (sex and age).
Men – 248 (57,5%), women – 183 (42,5%). Adults – 55% (predominate over children), children – 45%. There are some other classifications divided into six groups as follows:
| year | frequency | percentage | |
| 2007 | 46 | 10,7 | |
| 2008 | 66 | 15,3 | |
| 2009 | 40 | 9,3 | |
| 2010 | 47 | 10,9 | |
| 2011 | 46 | 10,6 | |
| 2012 | 72 | 16,7 | |
| 2013 | 74 | 17,2 | |
| 2014 | 40 | 9,3 | |
| total | 431 | 100,0 | |
Table №2 Age division by groups
According to aetiology of fresh burns the relation is as follows:
| Age | Frequency | Percentage | Total percentage |
| 0-3 | 45 | 10,4 | 10,4 |
| 4-10 | 73 | 16,9 | 27,4 |
| 11-18 | 77 | 17,9 | 45,2 |
| 19-35 | 98 | 22,7 | 68,0 |
| 36-65 | 109 | 25,3 | 93,3 |
| over 65 | 29 | 6,7 | 100,0 |
| total | 431 | 100,0 |
Table №3 Aetiology of fresh burns
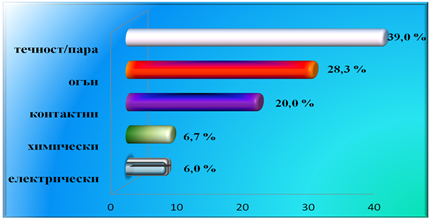
In children the most common reason for formation of post-burn hypertrophic scars is hot scald burns (47,17% of the children), and in adults – flame burns (32,62% of the adults).
Most rare are chemical burns in children (2,05%) and electrical burns in adults (4,23%). There is a statistically significant difference in the electrical burns and the age – almost 58% Р<0,05 (χ²=83,738) of the patients are at the age of 11-18 as well as in the aetiology and the sex – men injured by electrical burns are 92,7% Р<0,05 (χ²=20,476).
According to localization the most frequent surgeries are on the upper limb, the head and the lower limb.
Table №4 Division by localization

The damages are mainly on the upper limb (37,2%), followed by the damages on the head (face and capilitium) and the ones on the lower limb. Another localization is the neck (6,9%). Post-burn consequence on the body have been observed in 14,4 % of the patients. We examined particularly the axilla because of its specific localization and surgical approach – (6,9%).
The number of patients with more than one localization is 75 (17,4%). Both upper limbs of 44 (58,66%) of them are damaged and the difference is statistically significant Р<0,05 (χ²=11,297). 27 of these 44 patients are children.
The hospital stays are divided into short, medium and long-lasting. In most cases of PNL the hospital stays are short (52,7%) and the difference is statistically significant Р<0,05 (χ²=24,323).
Table №5 Number of hospital days
| Duration | Frequency | Percentage | Cumulative percentage |
| Up to 5 days | 227 | 52,7 | 52,7 |
| 5-10 days | 116 | 26,9 | 79,6 |
| Over 10 days | 88 | 20,4 | 100 |
| Total | 431 | 100 |
In 22 (5,1%) of the observed patients we found keloids, in 127 (29,5%) — contractures and in 30 (7,0%) syndactylies.
During our study we observed 30 (7,0%) syndactilies, 27 of which are on the upper limb, and the rest are on the lower one. 23 (11,8%) of the patients are children and only 7 (3%) are adults.
We observed keloids in 12 (54,54%) children and 10 (45,45%) adults and cotractures in 127 cases (29,5%) Р<0,05 (χ²=24,971).
More affected by this post-burn complication are the children. 81 (41,5%) of 195 children have contractures Р<0,05 (χ²=23,043).
In adults the difference is not statistically significant, but as compared to children it is of statistic significance Р<0,05 (χ²=24,971), where children prevail upon adults.
We found keloids in 5,1% (22 patients) – 12 (6,2%) children and 10 (4,2%) adults.
As regards the number of surgeries – 25 patients (55,6%) undertook two surgeries, 9 patents (19,98%) — three surgeries, 5 patients (11,1%) — four surgeries, 3 (6,66%) — five surgeries, two patients – 6 surgeries (4,44%) and solely one of the patients undertook 10 surgeries (2,22%).
We analyzed the results on the basis of the types of surgical techniques, the usage of which are shown in the table below:
Table №6 Types of surgical techniques
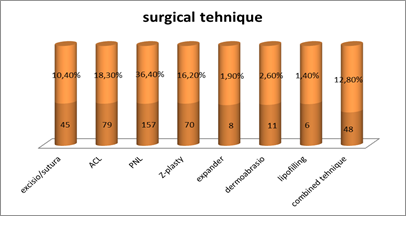
We analyze the Z-plasty separately from the free skin plasty because of its frequent use.
Age division of the patients based on the type of the used surgical method
Table № 7 Division by age and surgical method
| Surgery | Ex.sutura | ACL | PNL | Z-plasty | Expander | Comb. Technique |
| Children | 13% | 45% | 41% | 70% | 50% | 47% |
| Adults | 87% | 55% | 59% | 30% | 50% | 53% |
| % | 100 | 100 | 100 | 100 | 100 | 100 |
In Z-plasty we found statistically significant difference – children are three times more as compared to the adults Р<0,05 (χ²=22,862). In the other surgical methods there is no such a relation.
Table №8 Relation between surgical method and aetiology
| Surgery | Ex.sutura | ACL | PNL | Z-plasty | Expander | Comb.tehnique | |
| Flame | 6 | 27 | 44 | 17 | 2 | 23 | 119 |
| Scald | 18 | 34 | 60 | 27 | 1 | 25 | 165 |
| Electrical | 2 | 4 | 11 | 3 | 3 | 3 | 26 |
| Chemical | 5 | 6 | 13 | 1 | 0 | 3 | 28 |
| Contact | 14 | 8 | 29 | 21 | 1 | 9 | 82 |
Irrespective of the aetiology of fresh burns the basic surgical method is the PNL (local flaps and Z-plasty).
There is a statistically significant difference when comparing the data concerning sex and aetiology. Electrical injuries are observed in 92,3% of the men and only in 7,7% of the women.
In all cases of different localization the main surgical technique is local flaps. Only in cases located on the axilla we mostly used split-thickness skin graft.
Table №9 Relation between the localization and the surgical technique
| Ex.sutura | ACL | PNL | Z-plasty | expander | dermabrasio | lipofilling | Comb.tehnique | |
| Head | 17(19,10%) | 4(4,5%) | 48(53,93%) | 4(4,5%) | 4(4,5%) | 2(2,24%) | — | 10(11,23%) |
| Neck | 3(9,1%) | 1(3,03%) | 11(33,33%) | 7(21,21%) | — | — | — | 11(33,33%) |
| Upper limb | 7(3,84%) | 37(20,32%) | 53(29,11%) | 44(24,17%) | 2(1,09%) | 4(2,19%) | 1(0,42%) | 34(18,68%) |
| Body | 10(14,08%) | 14(19,71%) | 17(23,94%) | 10(14,08%) | 1(1,4%) | 2(2,81%) | 2(2,81%) | 15(21,12%) |
| Axilla | 5 (20%) | 6 (24 %) | 4 (16%) | 3 (12%) | — | — | — | 7 (28%) |
| Lower limb | 5(5,32%) | 26(27,66%) | 30(31,92%) | 9(9,58%) | 2(2,13%) | 4(4,25%) | 5(5,32%) | 13(13,82%) |
| More than one localization | 2(2,56%) | 19(24,35%) | 21(26,92%) | 12(15,39%) | 1(1,28%) | 1(1,28%) | 3(3,84%) | 19(24,35%) |
When using PNL we observe the shortest duration of hospital stay, which we find statistically significant (68,15%) Р<0,05 (χ²=24,323).
The difference between PNL and the treatment of keloids and syndactyly we find statistically significant. Z-plasty is the basic technique in treatment of contractures. In surgeries of the upper limb 42,4% (53 patients) the used technique is local and distant flaps.
Table №10 Complications according to the surgical technique
| Complications | Number | Re-surgery |
| Expander technique | 1 | 1 |
| Loss of STSG or FTSG | 1 | 0 |
| Epidermolysis | 8 | 0 |
| Partial necrosis of a flap | 7 | 3 |
| Recurrence of a keloid | 1 | 0 |
| Recurrence of a contracture | 4 | 2 |
| Recurrence of a syndactyly | 2 | 2 |
In the cases of complications when patients were not operated they were treated conservatively practicing monitored secondary epithelization. In cases of re-surgery of the complications we used flaps and skin-grafting.
Discussion
The treatment of the trauma should start in its earliest stage and last long after the end of the basic recovery process, in order to reduce the extend of the post-burn consequences (6). We should analyze it with respect to its complexity, concerning its functionality and its aesthetic side as well, which is of great importance as regarding the social adaptation of the patients.
There are different controversial opinions about the surgeries of hypertrophic scars. Brown believes that the surgery should be done as early as possible after the formation of the scar (7). On the other hand Limberg claims thet the early treatment of immature scars leads to recurrences and more contractures (9).
Taking into consideration the higher percentage of the contractures we practiced early surgical treatment during the first year after the trauma in cases of contractures, microstomia and ectropion. In all other cases we undertook surgical corrections averagely 2 years after the trauma.
The percentage of children with post-burn consequences is 45% (189), and in 77 (40,7%) of the cases we found contractures leading to various locomotory restrictions. In children the most common localization is the one on the upper limb (97) 51,3%, which fact reaffirms the oppinion of Barhudarova that in 40-60% of the hypertrophic deformations in children functional disorders are observed as well (1). According to Povstyanoy (5) contractures are the most severe post-burn complication and they are about 3-10% in adult patients. According to our data contractures are 127 (29,5%). At the age of 0-3 over 50% of burns lead to contractures. The largest number of contractures — 33 (42,8%) is observed in children at the age of 4-10.
Table №11 Contractures in children by localization
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||
Zavyalov shares the same opinion and claims that merely every hypertrophic scar in early childhood soon or later leads to functional or positional changes of the body (3). The risk of functional complications reduces the older patients go.
In adults contractures are 19,5% (46) , most at the age of 19-35.
The division by age is approximately equal at all age groups. We absolutely agree with the opinion of Hadjiyski that in cases of fresh burns and of post-burns as well the number of men is larger than the number of women (6).
Any plastic surgery method requires treatment of the neighboring tissues in spite of the used surgical method. Evstatiev believes that classification and planning of surgical approach may be determined according to the form of the defect independently of the localization (2).
212 (89.9%) of the adults were operated using basic surgical techniques (STSG, FTSG, PNL, expander technique, aesthetic procedures such as lipofilling and dermoabrazio) and 24 (10,2%) — using combined methods containing one-stage surgical techniques. In children we observe similar results — 160 (84,7%) using the basic techniques and 29 (15,3%) the combined ones. Hop and Prasad (8,11) reach similar results during their long-lasting study on fresh burns and post-burn consequences. Both of them report about a larger percent of contractures (over 72%) and most of them (over 50%) are on the upper limb. As opposed to our study Hop (8) observes more defects on head and neck.
As regards to the surgical technique we used the variations of PNL. Most common in adults are the local flaps and in children – the Z-plasty. The combined techniques including Z-plasty are most frequent with STSG (3,5%) and local flaps ( 3,9%) (2).
Z-plasty we analyze separately from the PNL because of its often usage.
This technique interrupts the brides. We use it in cases of tissue insufficiency in some areas. We agree with McGregor (10), who claims that the Z-plasty is the most effective surgical method.
We found significant difference in the frequency of cases of syndactyly – 7,65% according to our study and 19% according to Hop’s analysis. There is a difference in the age as well – in our study the percentage of children with such deformation is much larger and we use free skin transplant in three cases. Hop and Prasad use FTSG and STSG in 20% of syndactyly cases (8,11).
We used classic expander technique basically in cases of post-burn alopecia and a couple of cases of vitious deformations of the neck, forearm and lower limb. We agree with Zanzov (4), who claims that expander technique leads to good functional and aesthetic results in cases of post burn alopecia using skin, similar by color and elasticity and preservation of the left hair follicles. (4). We keep the same the ratio 2:1 (as Sasaki does) (12) between the expander size and the defect size.We agree with Hadjiyski about the aetiology of fresh burns – scald burns and flame burns are the most common cases of fresh burns and of post-burns as well (6).
Conclusions
The hypertrophic scars after burn injuries are very common. The patients need a varied treatment using surgical and conservative methods in order to provide them a good quality of life.
Bibliography
1.Бархударова, Нанна Рафаэльевна — 14.00.35 — Москва, 2009 ОПовышение эффективности хирургической реабилитации детей с послеожоговыми рубцовыми деформациями и контрактурами суставов конечностей с использованием реконструктивно-пластических операций
- Евстатиев Д. Покриване на дефекти по повърхността на тялото с местна пластика Автореферат към дисертационен труд 1977г.
3.Завьялов П. В. Ожоги у детей., Москва 1972.
- Зънзов Е. Оперативно поведение за възстановяване на тъканни дефекти при откритите травми на главата, Дисертационен труд март 2015г.
- Повстяной Н.Е., Восстановительная хирургия ожогов, Москва 1973г.
6.Хаджийски О. Изгаряния и измръзвания Академично издателство „Проф. Марин Дринов“ София 2008г.
- Brown J.B. The treatment of the late burn wounds and its contractures; On burns. Sprinfield- Illionis, 1953, p. 120
- Hop M.J. a,b, Langenberg L.C. c, Hiddingh J., C.M d. Stekelenburg b,c, M.B.A. van der Wal b,c, C.J. Hoogewerf a,b, M.L.J. van Koppen a, S. Polinder e, P.P.M. van Zuijlen b,c,f, M.E. van Baar a,e,*, E. Middelkoop Reconstructive surgery after burns: A 10-year follow-up study
- Limberg, A. A. (1946). Mathematical principles of local plastic procedures on the of the human body. Leningrad : Medgis.
10.Mcgregor IA.The theoretical basis of the Z-plasty. Br J Plast Surg 1957;9(4):256–9.
- Prasad JK, Bowden ML,Thomson PD.A review of the reconstructive surgery needs of 3167 survivors of burn injury.Burns 1991;17(August (4)):302–5.
- Sasaki GH ;Tissue expanders and general guidelines for tissue expansion technique. In Tissue Expansion in Reconstructive and Aesthetic Surgery. St. Louis, Mosby, 1998, pp 11-14[schema type=»book» name=»SURGICAL BEHAVIOR OF PATIENTS WITH POST-BURN CONSEQUENCES AN 8-YEAR STUDY» description=»Burn consequences in children as well as In adults are aesthetic imperfections and functional deficiencies at the same time. During our 8-year retrospective research we analyzed 431 surgical patients with hypertrophic scars and keloids. We looked through the results taking into consideration sex, age, aetiology, number of occupant days, localization, operation technique, number of surgical interventions, cases of syndactyly, keloids or contractions. When all the data was generalized we ascertained that surgical treatment was the basic approach to these defects and the basic surgical method were flaps (PNL). The injuries are most severe in children. That is why we consider the moment of surgical corrections and the surgical methods crucial for the best functional and aesthetic result.» author=»Dr. Vania Anastasova, Dimitar Evstatiev, Elean Zanzov» publisher=»БАСАРАНОВИЧ ЕКАТЕРИНА» pubdate=»2017-01-05″ edition=»ЕВРАЗИЙСКИЙ СОЮЗ УЧЕНЫХ_30.11.16_31″ ebook=»yes» ]