
INTRODUCTION
Joint replacement (alloplasty, endoprosthesis) of the hip joint is currently one of the most successful surgery procedures in orthopedics and traumathology. The exceptionally good results of this intervention over the past years have resulted in its worldwide implementation and application, which in turn leads to an increasing number of patients with hip joint endoprosthesis [5,40-480,11,68-72].
The physical and rehabilitation treatment plays an important role not only for the speed but also for the degree of the functional recovery of the patients with hip joint alloplasty [6,145-146]. Conducting the rehabilitation properly and in a timely has a significant impact on the quality of the recovery and also for the prevention of complications [8,3-14].
The aim of this study is to analyze the results of the Applied protocol for complex rehabilitation of patients with hip joint alloplasty during the early post-surgery period (the hospitalization period in an orthopedics clinic between the 2nd and 12th day after surgery).
METHODS AND MATERIALS
A total of 203 patients (135 female and 68 male aged 22 to 84) participated in the study. All of them underwent hip joint endoprosthesis surgery due to femoral neck bone fracture at UMBAL “d-r G. Stranski” in Pleven and had early rehabilitation under the supervision of specialists from the Clinic of physical and rehabilitation medicine (CPRM) between 2010 and 2014. For the purpose of the study, when starting the rehabilitation program during the second day post-surgery we performed the DAL test developed by H. Rusk (1964) for “putting on clothes and shoes” and “outfit and personal hygiene” (going to the bathroom, washing and wiping hands and face, brushing teeth, hair combing and shaving (for men) as well as a locomotion test (number of steps required per 10 meters, movement speed and distance) [13,29-32;4,93-99]. The methodics of the applied rehabilitation program have been developed at the CPRM around 30 years ago, and has been constantly improved over the years. The length of the procedure in the beginning is 5-10 minutes and reaches 15-20 minutes at the end of the observed period, and it’s performed once or several times daily according to the individual ability of each patient and includes KT and ET.
- Kinesitherapy procedures begin immediately after the surgery procedure and transferring the patient to the hospital room with “positional therapy” – the affected limb is placed in an adduction cast 10-15о in neutral position regarding the rotations [7,14-18;9,643-686;10,172-187].
In order to prevent post-surgery dislocation of the endoprosthesis joint, the patients are educated regarding the movements and activities from the different DAL that should be avoided and the precautions that should be taken. Isometric exercises are added on the second day post-surgery for the glueteal and hip muscles in a circulatory 1:1 regime aiming for improving the local blood circulation, overcoming the stasis and the post-surgery swellingthrough stimulation of the blood pump. Patients are shown breathing exercises that focus on the expectoration and cough reduction in order to overcome the effects of the anestesia and to prevent post-surgery atelectasis and pneumonia. Active physical exercises against resistance of the shoulder girdle, upper limbs and the contralateral limb are included. Patients train their balance from the permitted starting positions with both open and closed eyes. On the third day after the drainage removal the cast is removed as well and is replaced by an adductor orthosis.
Isometric exercises are included in the rehabilitation program for the gluteal and hip muscles in hypertrophic mode 1:4 in order to improve the trophics of the muscles based on the reactive hyperemia after contraction. Active exersises for the fingers and the ankle joint are recommended for the endoprosthesis limb from a lying down starting position (for prevention of vein stasis, thrombus formation and the risk of pulmonary embolism) in an open kinetic chain; mobilization of the patella (the patella dance); assisted exercises for flexion of the knee and hip joints with sliding of the patella while avoiding flexion of the hip joint with an extended knee due to the strong forces that apply on the joint [7,14-18]. The gradual mobilization of the reconstructed hip joint should be performed within the allowed volumes with moderate strength. Active assisted exercises within the allowed movement volumes should be performed within the confines of the bed with the patients laying on their back. Extra attention should be paid to the training of the m. quadratus lumborum, without manual resistance for elevation of the pelvis in order to prepare the patients for walking without leaning on the operated limb. Various techniques from the proprioceptive neuromuscular facilitation (PNMF) are included to ease the strain on the weak muscles of the operated limb and to overcome the muscle inhibition during the first days after surgery [9,643-686]. Elastic socks should be worn and the patients should train switching from laying on their back to a sitting position to prevent thromboembolic complications, and patients should be monitored for possible vascular vegetative reactions. The patients stand upright with individually adjusted crutches and the weight is shifted to the healthy limb, while the operated one should be held in adduction of around 30о [12,16-19]. Active exercises for flexion and extension of the knee joint and for balance and coordination should be performed from a standing starting position with a neutral position of the hip joint. Walking exercises begin after achieving orthostatic adaptation (4-5th day post-surgery). During the first day, the patients walk only inside the hospital room with a gradual increase of the time and distance. Training in climbing stairs is done only after the gait is stabilized on flat terrain according to the following routine: “healthy limb – crutches – operated limb” [1,598-618]. Going down the stairs follows the same pattern as walking on flat terrain.
- ET consists of putting on clothes and shoes, preparing an outfit and maintaining personal hygiene. To facilitate these activities, suitable clothing is recommended (wearing a night gown, no underwear).During the first few days post-surgery the patient is equipped with a urethral catheter, and the outfit is performed on a bedpan in the patient’s bed – the patient lies down on the side of their healthy limb with an adductor orthosis (pillow) between the knees. After that the patient lies back on their back with slightly flexed knee joints and adducted hip joints (the orthosis is removed), while removing the bedpan happens in reverse order. External rotation of the hip joint should be avoided as it involves risk of luxation. Maintaining genital hygiene and avoiding pressure of the skin on the upper and lower backside are necessary against decubitus wounds, especially for patients in an advanced age or overweight ones [2,10-14]. The patient returns to going to the bathroom (WC) around the 6th or 7th day if the verticalization process and the walking with aids training are going according to plan. Sitting on the toilet is performed through shifting of the operated limb in slight adduction without rotation. Getting up from the toilet is done with the help of the crutches, and the weight is shifted to the healthy lim. The patient is trained to avoid rotation with steady feet – for example when raising the lid of the toilet or when flushing. These activities are performed by moving the entire body in the respective direction [13,29-30;3,159-169]. Washing and wiping hands is performed with the crutches tucked under the armpits and following the aforementioned instructions. Washing the face and teeth requires both hands, so the patients stand on their healthy limb and rests the crutches against the wall with the operated limb only touching the floor slightly [10,172-197].
RESULTS
The results from the performed tests and measurements are stored in a custom individual file for each patient. To analyze the obtained data, we applied parametric methods – the T-test by Studant and the F-criteria by Fisher (ANOVA), as well as non-parametric methods for asymmetrical distribution – the χ2 test by Pearson, the W-test by Mann-Whitney (Wilcoxon) [14,183-184]. The values shown are from the initial tests (on the second day post-surgery) and upon discharge of the patients from the clinic.
Figure №1 displays the median arithmetic values (X) from the measured number of steps required per 10 meters and shows that the number of steps decreases with the improvement of the overall condition of the patients.
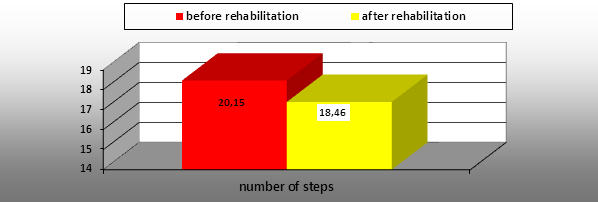
Fig. №1 Results from the number of steps required at the beginning and at the end of the observed period
Fig. № 2 shows the results from the median arithmetic values (X) of the movement speed for a distance of 10 meters at the beginning and at the end of the observed period. The time required by patients to walk 10 meters (measured in seconds) decreases, which points to an improvement in their functional condition.

Fig. №2 Results for the movement speed of patients at the beginning and at the end of the observed period, measured in seconds.
Fig. № 3 presents the Wilcoxon curve for the median arithmetic values (X) of the DAL test at the beginning and at the end of the rehabilitation period.
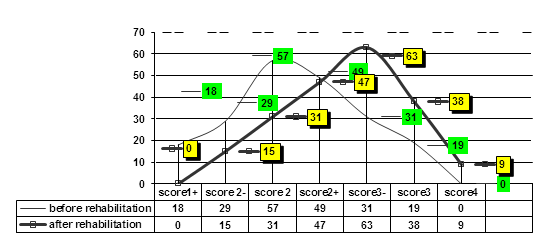
Fig. №3 Results from the DAL at the beginning and at the end of early rehabilitation.
CONCLUSIONS
- Performing rehabilitation for patients with hip joint alloplasty during the early post-surgery period helps with mobilizing the reconstructed limb, early verticalization, prevention from vascular and circulatory thromboembolic complications and eases the pain symptoms.
- The decrease the number of steps required and the increase of the walking speed suggest an improvement of the locomotion of the rehabilitated patients and an improvement in their functional condition.
- The presence of a peak and the shift of the Wilcoxon curve to the right upon discharge of the patients from the hospital shows an improvement in the self-service levels for the majority of them.
SUMMARY
Early rehabilitation of patients with hip joint endoprosthesis leads to a faster and more complete recovery and improves the functional mobility of the operated limb. Conducting early ET ensures independence of the patients in their daily activities when they return home, and benefits their psycho-emotional balance and self-esteem. A tangible improvement is observed in the recovery of the autonomy and self-service of the patients, along with reduced depression states.
REFERENCES
- Brander V., Srulberg SD. Rehabllitation after hip- and knee- joint replacement: an experience- and evidence-based approach <0 care, Am J Phys Med Rehab, 2006; 85(suppl. II): 598-61
- Bukowski EL. Practice guidelines: acute care management following total hip arthroplasty (postoperative days 1-4). Orthop Phys Ther Pract, 2005; 17(3):10-
- Cichy B., Wilk M., Sliwinski Z. Changes in gait parameters in total hip arthroplasty patients before and after surgery. Medical science Monitor, 2008; 14:159-169.
- Cook C., Hegedus E. Orthopedic physical examination tests: an evidence-based approach, Upper Saddle River. N). Pearson Prentice Hall, 2008, 93-
- Donatelli R, Wooden MJ. Оrthopaedic physical therapy, fourth edition, by Churchill Livingnone, an imprinl of Elsevier Inc., 2010, 400-480.
- Dreinhöfer et al. (eds.). EUROHIP: Health Technology Assessment of Hip Arthroplasty in Europe, EFORT Appropriateness of Total Hip Replacement K. Dreinhöfer Department of Orthopedics, Ulm, 2011, 55-63; 145-146.
- Ilieva E. Features of rehabilitation and occupational therapy after hip arthroplasty. Physical medicine, rehabilitation, health. 2007; 6 (4): 14-18 [In Bulgarian].
- Jotov A., Rusimov V. Current Aspects in Hip and Knee Joint Replacement. Physical medicine, rehabilitation, Health. 2013, 2:3-14 [In Bulgarian].
- Kisner C., PT, MS Therapeutic Exercise F. A. Davis Company 1915 Arch Street Philadelphia, PA. 2007, 191-03; 643-686.
- Maxey L. Rehabilitation for the postsurgical orthopedic patient Library of Congress Cataloging in Publication Data, 2001, 172-187.
- Tivchev P, Kinov P. et al. Arthroplastik of the Hip Joint. Sofia: BG Kniga, 2014; 37-57, 68-72 [In Bulgarian].
- Troev T, Milanova H, Mavrova R. Our experience in kinesitherapy after knee endoprosthesis. Medicine and sports2011; VII/ 4:16–19.
- Vacheva D, Mircheva A. Medical rehabilitation and occupational therapy of patients with hip joint arthroplasty (early postoperative period). Management and Education, 2013; ІХ (5): 29-32 [In Bulgarian].
- Velkova D. Health and social problems of the elderly people living alone in the villages. Pleven, 2000,183-184 [In Bulgarian].[schema type=»book» name=»RESULTS FROM A COMPLEX REHABILITATION PROGRAM FOR PATIENTS WITH HIP JOINT ENDOPROSTHESIS, APPLIED DURING THE FIRST TWO WEEKS AFTER SURGERY» description=»Introduction: Joint replacement (alloplasty, endoprosthesis) is currently one of the most successful surgery procedures in orthopedics and traumathology.The aim of this study is to track and measure the results of the administered protocol from the applied rehabilitation during the early post-surgery period (the hospitalization time in an orthopedic clinic from the 2nd to the 12th day after surgery) for patients with hip joint endoprosthesis. Methods and materials: A total of 203 patients (135 female and 68 male aged 22 to 84) with hip joint endoprosthesis due to femoral neck bone fracture participated in the study. The rehabilitation program consisted of: kinesitherapy (active exercise; verticalization in several stages; training in walking with walking aids) and occupational therapy – daily life activities. Results from the locomotion test (number of steps per 10 meters and movement speed) and from the Daily Activities of life test were taken at the beginning and at the end of the period. The results are stored in an individual file for each patient. Results and discussion: The statistical analysis of the results for number of steps per 10 meters and for movement speed show significant improvement of the overall functional condition of patients at the end of the hospitalization period. At the end of the early rehabilitation period, the Wilcoxon curve for the DAL test shifts significantly to the right, which signifies a better self-sufficiency for patients, as well as an improvement in their psychological and emotional state and well-being.» author=»Krastanova Maya, Valeshkov D.A., Vacheva D. E.» publisher=»БАСАРАНОВИЧ ЕКАТЕРИНА» pubdate=»2017-01-09″ edition=»euroasia-science.ru_29-30.12.2015_12(21)» ebook=»yes» ]