
Introduction:
Meckel’s diverticulum is a relatively common abnormality of the gastrointestinal tract, occurring in 2% of the normal population. The disease is usually asymptomatic, but can be presented with undefined abdominal pain [5]. The complications besides peptic ulceration, perforation, enteroumbilical fistula, intussusception and hemorrhage include the development of carcinoids and inflammatory pseudotumor.
Case report
Anamnesis: 61 years old male complaining of pain in the right abdomen was admitted to the surgical ward of the hospital – Svilengrad. The pain began two days ago. In the beginning it was diffuse and subsequently was localized in the ileocecal region, accompanied by nausea and vomiting.
Physical examination: The abdomen was on the level of the chest. The right half of the abdomen did not participate normally in the breathing movements. There was palpable pain in the ileocecal region. The palpation showed signs of peritoneal irritation and muscular defence. Bloomberg / + / positive. Liver and spleen were not palpable. There was preserved intestinal motility.
Diagnostic and therapeutic procedures: X-ray — no free gas collections under the diaphragm. Ultrasonography of abdominal organs — multiple small calculi into the gall bladder, single simple cyst in the left kidney, no evidence of enlarged lymph nodes and ascites.
Laboratory results: leukocytosis, elevated ESR, slightly elevated AST and ALT, no other deviations from the norm.
Surgical intervention: During the opening of the the abdominal cavity outflowed moderate amount of clear serous exudate. Appendix was flegmonously inflammed, covered with a fibrin coating and adhesions with the surrounding tissues were found. Typical appendectomy was performed. The revision of the small intestines revealed Meckel’s diverticulum, 10cm in length, with tubular shape, located 50 cm from the ileocecal valve, with own meso and catarrhal inflamed wall. A partial resection of the small intestine was performed, including the Meckel”s diverticulum.
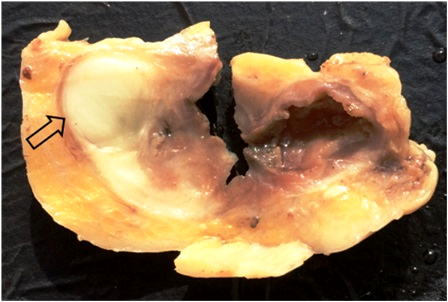
Material and metods: Histologic speciments were made with fixative of 10% neutral formalin and embedded in paraffin. The cut sections were 7 mkm thick and stained with hematoxilene and eosin (HЕ). Gross examination of the appendix showed hyperemia of the serosa and whitish exudate in the lumen of appendix. The Meckel’s diverticulum has 10cm in length. The cut surface revealed yellowish nodule with diameter of 1,5 cm (arrow in fig. 1), subserouslly located.
Subserous nodule in the wall of Meckel’s diverticulum (Fig.1)
Microscopic investigation of the surgically removed tissue (Biopsy № 470-473 / 08-03-2015) revealed:
- Appendix – Specimen of transversal section of appendix lumen, filled with purulent exudates. Epithelium of the mucosa and glands with desquamative changes. Submucous space was infiltrated by neutrophilic leucocytes.
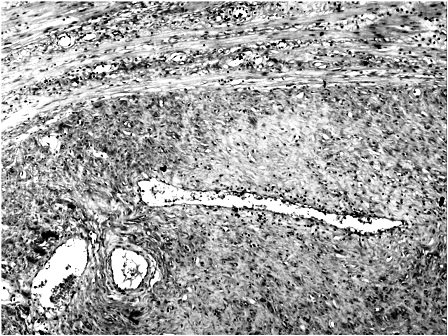
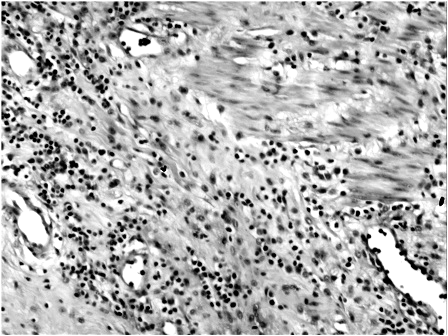
- Meckel’s diverticulum — The mucosa has ulcera The whole wall of the diverticulum – from mucosa to serosa was infiltrated by neutrophilic leucocytes. Subserously was found well encapsulated tumor-like formation (fig.2), which was composed of elongated myofibroblasts, containing abundant eosinophilic cytoplasm and vesicular nuclei, and fibroblastic spindle cells with inflammatory infiltration of neutrophils, eosinophils, lymphocytes, but few plasma cells. The stroma consisted of abundant blood vessels. There was no nuclear pleomorphism or atypical mitotic figures (fig.3)
Well encapsulated tumor-like formation, magn. x 40 (fig.2)
Benign inflammatory myofibroblastic tumor, magn. x 100 (fig.3)
The pathological diagnosis was: 1. Acute appendicitis; 2. Meckel’s diverticulum with phegmonous inflammation and benign inflammatory myofibroblastic tumor in the wall.
Postoperative period: The patient was clinically healthy, afebrile.
Disscusion
Inflammatory pseudotumor is a pathological process with plural localizations and unknown aetiology, but is supposed to occur secondary to infectious inflammatory processes [1]. It can develop in lungs, bone, head, larynx, mandible. The abdominal forms of IMT affect esophagus, stomach, liver, spleen [4], pancreas, the mesenterium, retroperitoneum, diaphragm, urinary bladder, kidneys, adrenal glands, small and large bowels, appendix and last – Meckel’s diverticulum [5]. In the described case the inflammatory myofibroblast tumor was found subserosally in the wall of a Meckel’s diverticulum. The second casuistic element is the patient’s age (61 years old), because nflammatory myofibroblastic tumor is more common in children and young people. The third element is the lack of clinical manifestations of the Meckel’s diverticulum for a long period of time. The reason for the surgical intervention of the patient was acute appendicitis and the inflamed Meckel’s diverticulum with ulceration of the mucosa and the subserosally located inflammatory myofibroblast tumor in its wall were accidental findings. In adult patients with symptoms of acute abdomen inflammatory myofibroblastic tumor and Meckel’s diverticulum should be considered in the differential diagnosis [2].
References
- Akhtar M., Gandhi D., Wilkinson A., Chandak K., Inflammatory pseudotumour of the jejunum presenting as intussusception. Journal of Dental and Medical Sciences (IOSR-JDMS), — Feb. 2013, Volume 4, Issue 6, p.17
- Bhattarai A., Poudyal S., Bhandari RS., Lakhey PJ., Singh KP., A Retrospective study of Intussusception of the bowel in adults. Journal of Institute of Medicine, April, 2015, 37:1
- Giovanni D. P., Stanley T. Leung, Pseudoneoplasms of the Gastrointestinal Tract. Arch Pathol Lab Med, March 2010, Vol 134 378
- Lamprini K., Khaldi L., Galani P.,Mytas D. and Lafoyianni S.. A rare case of an inflammatory myofibroblastic tumor in a middle-aged female, Case Reports in Oncological Medicine, Vol. 2012, Article ID 148053, p.3
- Wakefield S.E., Baigrie R.J., Molyneux A.J., Dowling B.L. Inflammatory pseudotumour in Meckel’s diverticulum producing intussusception. Br J Surg. 1995 Jan;82 (1):30-1.[schema type=»book» name=»Benign inflammatory myofibroblastic tumor in the wall of Meckel’s diverticulum» description=»Inflammatory myofibroblastic tumor, also called inflammatory pseudotumor, is a rare cause of obstruction and acute abdomen [3]. It occurs often in children but can occur at any age. Inflammatory myofibroblastic tumor is benign, but may recur. Rarely has malignant behavior. We report a case of 61-year old man who presented with abdominal pain and distending of abdomen since one day. The clinical diagnosis was acute appendicitis. During the surgical intervention was removed the inflamed appendix and was found the presence of Meckel’s diverticulum located 50 cm from the ileocoecal valve. The diverticulum was with tubular shape, 10cm length and inflamed serosa. A part of the small intestine including the Meckel’s diverticulum was removed. The morphological investigation revealed inflammatory myofibroblastic tumor inside the wall of the diverticulum. In adult patients complaining of sypmtoms of acute abdomen the inflammatory pseudotumor with intestinal localization should be considered in differential diagnosis.» author=»Vangelov Nasko Dimitrov, Ermov Dimitar Angelov, Bivolarski Iliya Petrov» publisher=»БАСАРАНОВИЧ ЕКАТЕРИНА» pubdate=»2017-01-30″ edition=»ЕВРАЗИЙСКИЙ СОЮЗ УЧЕНЫХ_31.10.15_10(19)» ebook=»yes» ]