
Introduction:
The history of the bronchial reversibility tests and knowledge starts at the end of the 1950s, when airway diseases were divided into reversible and non-reversible depending on the response to bronchodilator drugs. Despite the long history of the bronchodilator response (BDR) as a diagnostic tool still there are no commonly accepted rules for its performance. According to the latest statement paper of the ATS/ERS Task Force for standardization of lung function tests in 1995, there is no consensus on the molecule, dose and route of administration of a bronchodilator drug. [1] There is no clear consensus about what affects the reversibility in patients with bronchial obstruction.
The most common methods for expression of BRD are three: percentage of initial (baseline) value (pre-BD FEV1), percentage of predicted value (pred. FEV1), absolute change in mL. Original Bulgarian contribution, done by Kostianev and al. is the attempt to eliminate disadvantages of each one of the above-mentioned methods as the value to which the difference is presented as half-sum from the initial and the predicted FEV1 [2]. Using this equation all the elements which determine the intensity of BDR are taken into account. [3]
The contemporary consensus of ERS/AST accepts BDR as a positive when an increase in FEV1 of >12% and 200 mL in absolute value is noted without giving specific instructions to interpret the test in childhood. [1]. Less increase (<8% or <150mL) may very likely be due to natural variability of the measurement (intraspecific variability). Where the change is above this value, the next step is to determine the clinical significant threshold for positive BDR.[1]
Aim: The aim of our study was to define the clinical value of the BDR and to validate different cut-offs and methods for evaluation of the bronchial reversibility in asthmatic children.
Material and methods: For a period of 2 years (Oct. 2013 — Dec 2015) we evaluated medical history data of 211 children with asthma and 46 healthy children aged 5 to 17 years old. For all children, we performed pulmonary function tests (PFT) (pre- and post-bronchodilator spirometry), nasal smears for eosinophil counts, drew blood for IgE against inhalation and food allergies antibodies detection and ACQ* (Asthma Control Questionnaire), validated Bulgarian translation and ACQ interviewer-administered version for the age 6-10 years. We used SPSS v. 19. software. A p value of ,0.05 was considered statistically significant. *QOL TECHNOLOGIES Ltd 2003, Professor Elizabeth Juniper, www.qoltech.co.uk
Results:
There is no statistical difference in both groups for age, height, weight and BMI results, but there was difference regarding the sex distribution. In the control group the girls prevailed while in the group of children with asthma male was the predominant sex. Both initial output spirometry and BDR were significantly different between children with asthma and the healthy controls, as well as there was difference among asthmatic children when grouped according to the degree of decreased initial FEV1 (³80%, <80%³70%, <70%³60% and <60%).
Table 1
Patients demography and spirometry results
| Indicator | Healthy (N=48) | Asthma (N=211) | р | FEV1³80%
(N=128) |
<80% FEV1³70%
(N=32) |
<70%FEV1³60%
(N=19) |
FEV1 <60%
(N=16) |
р |
| Sex, male | 21 (39.3) | 134 (63.5%) | 0,022 | 83
(64,8%) |
25
(78,1%) |
8
(42,1%) |
9
(56,3%) |
>0,05 |
| Sex, female | 27 (60.7%) | 77 (36.5%) | 45
(35,2%) |
7
(21,9%) |
11
(57,9%) |
7
(43,8%) |
||
| Age, years.
Mean (SD) |
10,26
(2,98) |
10,18
(3,54) |
>0,05 | 128
(65.6%) |
32
(16.5) |
19
(9.7%) |
16
(8.2%) |
>0,05 |
| Height, cm
Mean (SD) |
144,75
(16,987) |
143,33
(18,660) |
>0,05 | >0,05 | ||||
| Weight, kg
Mean (SD) |
37,75
(13,645) |
40,61
(16,661) |
>0,05 | >0,05 | ||||
| BMI
MD (SD) |
17,34091
(3.90) |
18,87008
(3.00) |
>0,05 | 0,045 | ||||
|
Spirometry results (median, IQR) |
||||||||
| FVC | 91,8% | <0,0001 | 96,20% | 86,45% | 78,60% | ,62700 | <0,0001 | |
| FEV1 | 98,5% | 85,4% | <0,0001 | 91,25% | 76,15% | 67,30% | ,55250 | <0,0001 |
| FEV1/FVC | 91,5% | 92,1% | <0,0001 | 95,700 | 86,15% | 83,70% | ,55250 | <0,0001 |
| PEFR | 91,0% | 81,7% | <0,0001 | 86,40% | 70,00% | 64,10% | ,56150 | <0,0001 |
| MMEF25/75 | 99,5% | 52.3% | <0,0001 | 61,40% | 40,25% | 32,80% | ,26050 | <0,0001 |
| D FEV1%init. | 3.0% | 14,50% | <0,0001 | 11,50% | 17,16% | 26,80% | ,3430 | <0,0001 |
| D FEV1 abs., l | 0,050 | 0, 216 | 0,004 | 0,188 | 0,256 | 0,380 | 0,417 | <0,0001 |
For the studied population of asthmatic children, we calculated bronchodilator change in FEV1 using three basic formulas — as a percentage of baseline (ΔFEV1% init.), as a percentage of the predicted value (ΔFEV1% pred.) and as an absolute change in litres (ΔFEV1abs. change, L). There was a very good correlation between the three formulas. The most widely used in clinical practice formula — ΔFEV1% from baseline showed excellent correlation with ΔFEV1% of the predicted value (Spearman’s rho 0.859, p = 0.000) in the study population, which is why it was chosen to be used in our study. We found weak but significant correlation of BDR calculated as an absolute change (in mL), age, height, weight and BMI (Spearman’s rho ~ 0.3).
Using the method of ROC curves, a test is considered as a discriminatory (diagnostic utility) at an area under the curve (AUC) over 0.70. This method was applied in order to define the optimal threshold for positive BDR (ΔFEV1% init.), for discrimination, the asthmatic children from healthy controls with the best combination of sensitivity and specificity. AUC for BDR (ΔFEV1% init.) was 0.924 (95% CI 0,887-0,961). 6.15% threshold for positive BDO (ΔFEV1% init.) showed the best combination of sensitivity (82.8%) and specificity (100%) for the stated purpose.
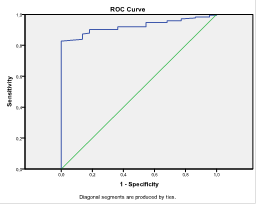

Figure 1 ROC curve for calculating sensitivity and of positive BDR cut-off 12% for discrimination the asthmatic children from healthy controls
We calculated lower sensitivity (60.9%) with high specificity (100%) for the “classic” cut-off for positive BDR (ERS/ATS; GINA) ≥12%. Cut-off ≥9% in the studied population is better than the one of ≥12% with 73% sensitivity and 100% specificity.
Using the method of ROC curves, we analysed new (alternative) criteria for BDR compared to the classical one (∆FEV1%init.≥12%) namely ∆MMEF25/75%init, ∆MMEF25/75abs., ∆FVC%init. and ∆PEF%init. All tested criteria (MMEF25/75, FVC, PEF) demonstrated good discriminative qualities for determining the children with positive BDR with AUC higher or equal to 0,7 (AUC>=0.7)
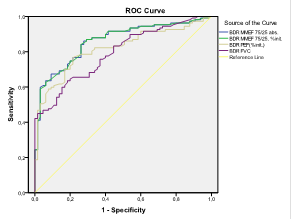

Figure 2 ROC curve for four alternative BDR criteria
The highest AUC (AUC=0,956, 0,860) is the bronchodilator change in MMEF25-75, calculated as a percentage of initial value and as an absolute change. The presentation of BDR as an absolute difference has a number of disadvantages in childhood due to dependency on this indicator of age, respectively, the size of the lung. Best threshold for a positive BDR calculated on ΔMMEF75 / 25,% init. is 29.9% (30%), which showed 84.1% sensitivity and 73.8% specificity, a positive predictive value (PPV) 84 and negative predictive value (NPV) 73,9.
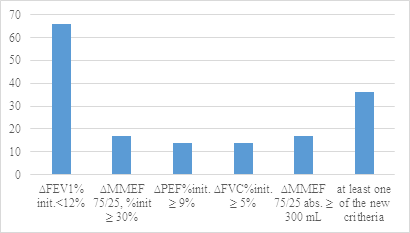

Fig 3 Children from the “non-responders” group with positive BDR according the new criteria.
We evaluated the children with negative BDR according the classical criteria (“non-responders”- 66 children) according the aforementioned new ones and found out 36 from them to have positive BDR in at least one of the parameters. The indicator ∆MMEF75/25%init ≥ 30% revealed additionally 17 more children (25,8%) from the “non-responders” group as children with positive BDR.
In order to determine whether the new diagnostic criteria are useful as an alternative to DFEV1% init.≥12% in children with mild and moderate asthma (FEV1≥80%), we conducted the same analysis for children with normal initial FEV1. We found the same thresholds for positivity and all tested indicators showed good discriminatory power (AUC> 0.7). Calculating as positive at least one of the new criteria we could reveal additional 30 children with positive BDR in the group of «non-responders» children with normal baseline FEV1.
Discussion:
The proof of bronchial hyperreactivity in the context of clinical symptoms provides further details in the mosaic of diagnosis and monitoring of childhood asthma. [4]. The demonstration of bronchial lability by measuring the response to inhaled bronchodilators in order to simplify the diagnosis and monitoring of asthma in childhood continues to represent scientific interest despite the long history of BDR. The «perfect» formula for expression of BDR should be independent of baseline FEV1 and to reflect the true response to the drug; to correlate well with the clinical response; to allow comparison between subjects with different baseline values and to provide information on the severity of post-bronchodilator obstruction. [5]
With correlation analysis, we found an excellent direct correlation between ∆FEV1 as a percentage of the initial value and ∆FEV1 as a percentage of the predicted value (Spearman’s rho 0.859, р=0.000) similarly to the published medical literature. [5-7] The most commonly used formula for calculating the BDR — ΔFEV1%initial depends significantly from baseline of FEV1[5]. This was confirmed in our study the ∆FEV1 %init. Is the most strongly influenced by the initial FEV1%pred. (Spearman’s rho=-0.567). Representing the BDR as an absolute difference has a number of disadvantages in childhood due to dependency on this indicator of age, respectively, the size of the lung. This is confirmed by our analysis that found weak but significant correlation of BDR calculated as an absolute change (in mL) with the age, height, weight and BMI (Spearman’s rho~0.3).
Therefore, the ΔFEV1%initial would have shown higher BDR in subjects with lower initial value of FEV1. Calculating the change in FEV1 according to the predicted value corrects the factors of age, height and gender, which all determine the size of the lungs. This formula, however, also has its drawbacks, because the calculation assumes that the estimated value is the maximum possible. In patients with baseline values of FEV1, greater than predicted, the calculation of BDR on ΔFEV1% predicted and ΔFEV1 [5] would show meaningless value. [5]
The validity of the most commonly used definition for positive BDR (ΔFEV1≥12%) is controversial for children. This threshold is significant clinically in adults with asthma and healthy controls. For the studied population of children with asthma and healthy controls we calculated AUC 0,924 (95% CI 0,887-0,961) for BDR (∆FEV1 %init.). Threshold of 6.15% for positive BDR (∆FEV1 %init.) showed the best combined results for both sensitivity (82.8%) and specificity (100%) for discriminating healthy children from those with asthma. We calculated lower sensitivity (60.9%) with high specificity (100%) for the “classic” cut-off for positive BDR (ERS/ATS; GINA) ≥12%. The most commonly discussed and studied in pediatric population cut-off ≥9% is better than the one of ≥12% with 73% sensitivity and 100% specificity. Our results are in accordance with the literature but with higher sensitivity. This higher result can be explained with the strict inclusion criteria used for our control group – only children with negative history for previous episodes of bronchial obstruction and allergic rhinitis.
As noted by the authors, conducting BDR studies in children before threshold of 9% for BDR as a diagnostic test for asthma in childhood to be imposed, it is necessary to conduct prospective unselected cohort of this indicator, because the diagnostic value may vary depending on the frequency of «wheezing»/asthma in this population.
BDR is a test with very high specificity, but relatively low sensitivity for confirming asthma diagnosis and probably it would have better clinical use in the childhood asthma management, especially before the initiation of therapy with inhaled corticosteroids (ICS) [8] High BDR is associated with poor control of the disease, increased exacerbation risk and presence of active inflammation of the airways, bronchial hyperreactivity and good therapeutic response to ICS. [9]
To evaluate the clinical significance of BDR for the different positive thresholds and its correlation to the clinical control of the symptoms and the risk factors we performed logistic regression analysis and analysis type “case-control study”. Our results are similar to those published before. In children with diagnosed asthma, independently from the initial FEV1 and the controller therapy, threshold of ∆FEV1%init.≥8% is associated with 2.369-fold (95% CI 1.077-5.213) higher risk for at least one hospitalization from the previous year and 2.871-fold (95% CI 1,239-6, 653) higher risk for school absence because of the asthma. The same correlation although weak is preserved in thresholds of BDR ≥9% and ≥11% with 2.282-fold and 2.159-fold for the hospitalization risk respectively. Children with BDR DFEV1%init.³10% have 3-fold higher probability for exercise exacerbation with OR 3.09 (CI 1.101-8.674). Classical threshold of ≥12% couldn’t predict the risk of hospitalizations, but is associated with 3.142 (95% CI 1,505-6,562) higher probability for school absence. In the study population, we didn’t find any relationship between BDR and atopic status of children (main groups of aero-allergens).
Similarly, to Galant et al. [9] In the group of children treated with ICS we found that BDR can reveal children with high risk using cut-off 12% and 11%, but not when using a lower threshold for significant BDR. In steroid naïve patients, we proved that BDR over 12% increases the likelihood of expression of at least one element of the risks 2.66-fold (95% CI 1,08-6,669).
The lack of consensus on the formula and the indicator that reflects the BDR leads to a number of studies in children and adults, conducted in demand to find the ideal threshold and the «ideal» parameter.
Castro et al. [10] conducted a comparative analysis of four alternative criteria for assessing the BDR [ΔPEF %; ΔFEF25-75%, ΔsGaw, ΔPEF (l) and ΔFEF25-75(l)] in adults with mild to moderate bronchial obstruction Three of the alternative criteria indicate AUC > 0.070 with a threshold of significant response very close to our calculations: ΔPEF≥8%; %; ΔFEF25-75≥27%, ΔsGaw≥25%, confirming their usefulness as criteria for positive BDR. As best threshold for ∆MMEF75/25 %init. we identified 29.9% (30%), which showed 84.1% sensitivity and 73.8% specificity, a positive predictive value (PPV) 84 and negative predictive value (NPV) 73.9. For ∆PEF%init. We defined threshold of 9.35% with an optimal ratio of sensitivity and specificity (76.6%, 85.4% respectively). Vilozni et al. [6] demonstrate sensitivity of post-bronchodilator increase in ΔFEF25-75%≥18.2% over 91.6% even in children with mild asthma. The positive response for FEF25-75% correlated with the severity of obstruction at all severity forms of asthma. The authors define a threshold for ΔFEV1 9.2% and 18.5% for ΔFEF25-75% as clinically significant BDR. Passerini et al. [8] found that BDR ΔFEF25-75≥25% distinguishes the best children with asthma from healthy ones with sensitivity 41% and specificity 80%. Best value for positive probability (positive likelihood ratio) according to the authors gives threshold ΔFEV0.5>11% (sensitivity 30% and specificity 90%).
Conclusion:
Pulmonary function tests are an important element of the study of respiratory diseases in children. They are sensitive and objective way to identify and evaluate the severity of pulmonary dysfunction, monitoring the progression of the disease and the evaluation of the therapy. BDR is widely used in confirming the diagnosis of asthma, but it can be a reliable method for monitoring and control of children with asthma. Establishing an adapted for childhood spirometry criteria in addition to the assessment of clinical symptoms, physical examination and determination of atopic status would improve substantially asthma control, making proper therapeutic decisions and identifying the risk of progressive loss of lung function.
Bibliography:
- Pellegrino R, Viegi G, Brusasco V, Crapo RO, Burgos F, Casaburi R, et al. Interpretative strategies for lung function tests. Eur Respir J. 2005;26(5):948-68.
- S K. A new approach to the evaluation of the bronchodilator response. Follia Medica. 1994;XXXVI:11-6.
- Благой Маринов СК. Бронходилаторен отговор и неговата многолика природа при ХОББ и бронхиална астма. InSpiro. 2011;14(2):20-4.
- Eigen H, Montgomery GS. Bronchodilator response: another piece in the asthma mosaic. J Pediatr. 2007;151(5):446-8.
- Chhabra SK, Vijayan VK, Gupta R, De S. Expression of bronchodilator response: comparison of four indices. Respir Med. 2002;96(8):611-4.
- Vilozni D HF, Livnat G, Bentur L. Forced expiratory decay in asthmatic preschool children—is it adult type? Respir Med 2013 Jul;107(7):975-80.
- H.J. Waalkens, van Essen-Zandvlietl,P.L.P. Brand, J. Gerritsen, E.J. Duiverman, K.F. Kerrebijn, K. Knol,Ph.H. Quanjer, and the Dutch CNSLD study group. Assessment of bronchodilator response in children with asthma. European Respiratory Joumal. 1993;6:645-851.
- Linares Passerini M, Meyer Peirano R, Contreras Estay I, Delgado Becerra I, Castro-Rodriguez JA. Utility of bronchodilator response for asthma diagnosis in Latino preschoolers. Allergol Immunopathol (Madr). 2014;42(6):553-9.
- Galant SP, Morphew T, Newcomb RL, Hioe K, Guijon O, Liao O. The relationship of the bronchodilator response phenotype to poor asthma control in children with normal spirometry. J Pediatr. 2011;158(6):953-9 e1.
- Castro A MP, Tavares B, Matos MJ, Segorbe-Luís A. Alternative functional criteria to assess airflow-limitation reversibility in asthma. Rev Port Pneumol (2006). 2015 Mar-Apr;21(2):69-75.
Corresponding author: Snezhina Lazova, MD snejina@lazova.com[schema type=»book» name=»MEASURING THE BRONCHIAL REVERSIBILITY IN ASTHMATIC CHILDREN» description=»Background: Despite the long history of the bronchodilator response (BDR) as a diagnostic tool, still there are no commonly accepted rules for its performance. Aim: The aim of our study was to define the clinical value of the BDR and to validate different cut-offs and methods for evaluation of the bronchial reversibility in asthmatic children. Methods: We performed lung function tests and BDR in 211 children with asthma and 46 healthy children and analyzed the results. Results: Threshold of 6.15% for positive BDR (∆FEV1 %init.) showed the best combined results for both sensitivity (82.8%) and specificity (100%) for discriminating healthy children from those with asthma. Cut-off ≥9% is better than the “classic” one o (ERS/ATS; GINA; ≥12%) with 73% sensitivity and 100% specificity. Conclusion: BDR is a test with very high specificity, but relatively low sensitivity for confirming asthma diagnosis and probably it would have better clinical use in the childhood asthma management, especially before the initiation of therapy with inhaled corticosteroids. » author=»Lazova Snezhina Mihaylova, Perenovska Penka Ilieva, Miteva, Dimitrinka Sabkova» publisher=»БАСАРАНОВИЧ ЕКАТЕРИНА» pubdate=»2017-01-13″ edition=»ЕВРАЗИЙСКИЙ СОЮЗ УЧЕНЫХ_30.12.16_33(2)» ebook=»yes» ]