
Introduction
Fractures in the hip joint area (fig. 1) are the worst complication of general osteoporosis and pose a serious threat to the health and survival of the elderly people.
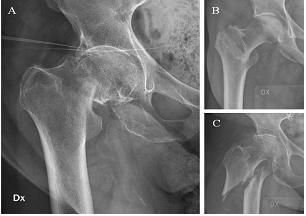

Fig. 1 X — Ray of Different Hip Joint Fractures
The number of hip joint fractures is increasing due to the prolonged lifespan of the population [1]. The risks of having such a fracture is determined by various factors like osteoporosis, previous fractures, impaired overall health conditions, cognitive impairments, changes related to age, and traumas [2].
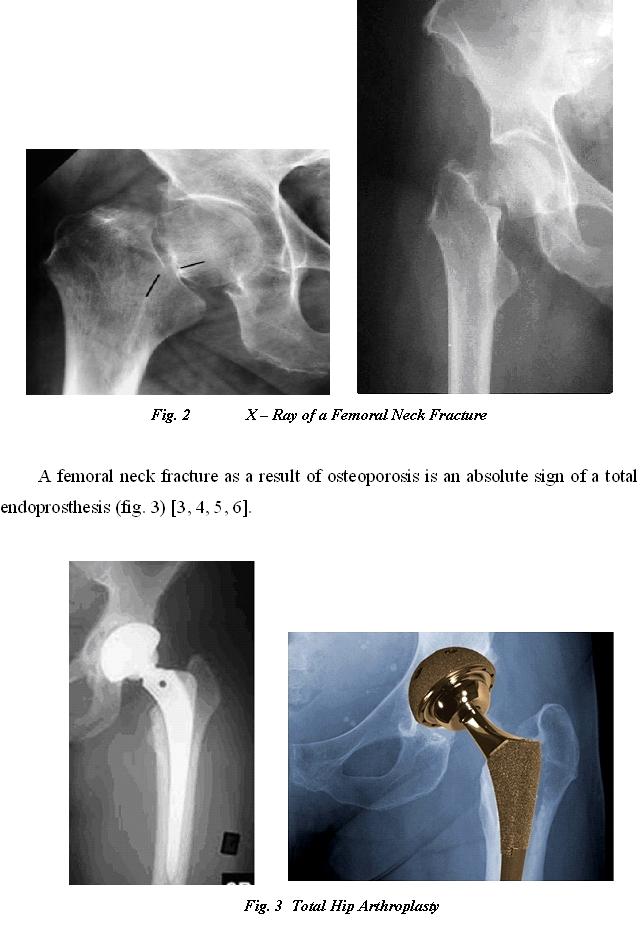
Approximately 50% of the hip joint fractures worldwide affect the femoral neck (fig. 2), while the rest are trochanteric and subtrochanteric fractures. Frandsen and Kruse (1983) predict that the number will triple (to 6, 5 million) by year 2050 [6, 7].

The degree of functional recovery of patients with hip joint arthroplasty is determined by the complex physiotherapy treatment program [4, 8], combined with prevention from further fractures. This is achieved by maintaining a good cooperation between the physiotherapy and rheumatology specialists.
Aim
The aim of this study is to present a combined approach of the Rheumatology Clinic and the Physical and Rehabilitation Clinic at the Univeristy Hospital in Pleven, Bulgaria, for treatment of patients with hip joint endoprosthesis after a femoral neck fracture as a result of general osteoporosis.
Methods and Materials
The target group for the study consists of 41 patients with hip joint endoprosthesis due to a femoral neck fracture, and all of them were diagnosed with general ostheoporosis using the osteodensitometry method. All patients had initial and final measurements and tests taken according to a specifically created individual patient file, which includes: a visual analog scale for the pain (VAS), goniometry, manual muscle testing (MMT), locomotion test, and a daily activities of life test (DAL).
The complex therapy includes drug treatment with bisphosphonates controlled by a rheumatologist, and a physiotherapeutic program which consists of: kinesitherapy, occupational therapy, electrotherapy with low frequency magnetic field (LFMF), interferential currents (IFC) and electrostimulation of the abductor muscles of the hip joint.
- Kinesitherapy – consists of an early stage and a later stage protective period (fig. 4), followed by a period of functional recovery which is custom designed for each patient (fig. 5) [11].
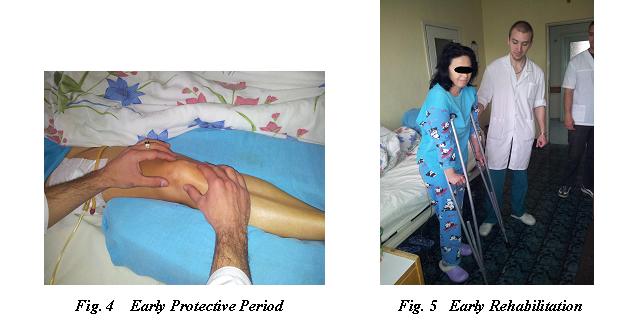

- Occupational therapy – performing daily life activities related to maintaining an outfit and personal hygiene, putting on clothes and shoes and other work- and transport-related activities [9, 10].
- Electrotherapy – LFMF ( 6) and IFC and electrostimulation of the abductor and protractor muscles of the hip joint (fig. 7).


Results
The data from the study was processed using two statistical computer programs – the Wilcoxon signed ranks test and SPSSS for Windows v.7.0. All the results from the initial and final measurements and VAS tests for the pain, goniometry, manual muscle tests, locomotion tests and DAL tests were used.
- The results of the VAS tests for pain are displayed on fig. 8, and show that the patients report significant pain immediately after trauma (11,33 points out of maximum 20), which impairs their overall psychological and emotional condition. At the end of the rehabilitation process the subjective feelings of pain are reduced to 2,57 points, which is very close to no pain at all (0 points).
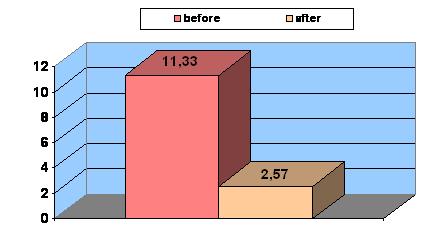

Fig. 8 Results of VAS for pain at the beginning and end of the recovery process
- The results of the locomotion tests are presented on fig. 9 and reflect the recovery of the patients’ ability to move with or without any walking aids at the end of the first year after endoprosthesis. It should be noted that at the beginning of the rehabilitation process, over 70% of the patients can only walk using two axillary crutches. At the end of the observed period around 75% of them are able to walk without any aids or just with one cane.
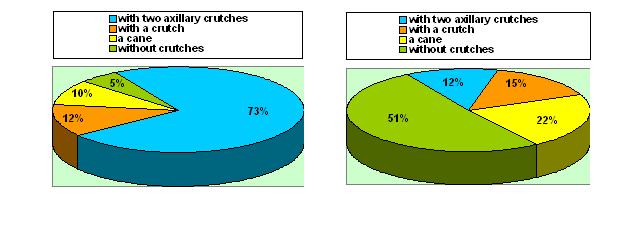

Fig. 9 Restoring the locomotion of endoproshtesis patients
- Figure 10 shows the Wilcoxon curve for DAL results from the beginning and the end of the rehabilitation process. At the end of the period the curve shifts to the right, which indicates an independent and unaided movement of patients with hip joint arthroplasty after a femoral neck fracture.
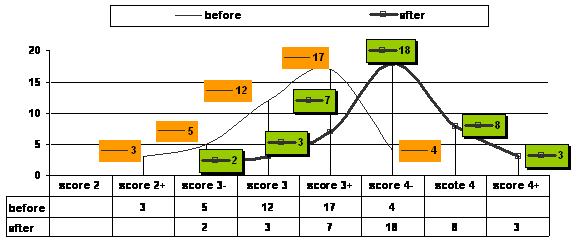

Fig. 10 Tthe Wilcoxon curve for recovery DAL
Implications
- The analysis of the results proves the need for a complex approach for treatment of patients with hip joint arthroplasty after a femoral neck fracture.
- This approach requires a systematic and phased physio-rehabilitation program and a continuous drug treatment for general osteoporosis.
Conclusion
A positive effect from the complex drug and physiotherapeutic treatment has been observed in all the measured indicators over the course of one year after endoprosthesis, regardless of the patients’ age and sex.
References
- Bhandari M. et al. Operative management ff displaced femoral neck fractures in elderly patients. An international survey. J Joint Bone Surg. 2005, 87 A:2122-2130.
- Frandsen P A., Kruse T. Hip fractures in the county of Funen, Denmark. Implications of demographic aging and changes in incidence rates. Acta Orthop Scand. 1983, 54:681-686.
- Johnell O., Kanis J A. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int. 2006, 17:1724-1726.
- Jotov A., Rusimov V. Current Aspects in Hip and Knee Joint Replacement. Physical medicine, rehabilitation, Health. 2013, 2:3-14 [In Bulgarian].
- Learmonth I D., Young C., Rorabeck C. The operation of the centery: total hip replacement. Lancet, 2007, 37:1508-1519.
- Tivchev P., Kinov P. et al. Arthroplasthy of the Hip Joint. Sofia, BG Kniga. 2014, 148-188 [In Bulgarian].
- Zachev N. Arthroplasthy of the Hip Joint. Sofia, BG Kniga. 2014, 337-343 [In Bulgarian].
- Vacheva D. Medical rehabilitation in patients with hip endoprosthesis. B: Arhipova L. XIX International Correspondence Scientific-Practical Conference «Innovations in Science» – «Modern medicine: current issues». 2013, Collection of materials. Novosibirsk: NP „SiBAK”, 77-87 [In Russian].
- Vacheva D., Mircheva A. Development Activities of the Office of Labor-and Occupational Therapy in KFRM at University Hospital » G. Stransky» Pleven. Health and science. 2012, vol. 2, (3) 430-436 [In Bulgarian].
- Vacheva D., Simeonova V., Stamenov B. The Recovery Detection of Daily and Labour Activities in the Everyday Life (Preparing Food and Feeding) in Patients who Suffered from Brain Vascular Disease. J of 2013, vol. 19, (3), 448-452 [In Bulgarian].
- Vacheva D., Mircheva A. Medical rehabilitation and occupational therapy in patients with hip endoprosthesis. Management and Education. 2013, ІХ, (5), 29-32 [In Bulgarian].[schema type=»book» name=»COMPLEX TREATMENT FOR PATIENTS WITH TOTAL HIP ARTHROPLASTY AFTER A HIP JOINT FRACTURE » author=»Krastanova Maya Stefanova» publisher=»БАСАРАНОВИЧ ЕКАТЕРИНА» pubdate=»2017-05-06″ edition=»ЕВРАЗИЙСКИЙ СОЮЗ УЧЕНЫХ_ 28.02.2015_02(11)» ebook=»yes» ]