
1.INTRODUCTION:
The modern diabetology explains clinical patterns of the continuum: metabolic syndrome (MS) –> non-insulino-dependent diabetes mellitus (NIDDM) –> diabetic polyneuropathy (DPNP) –> neuropathic diabetic foot (DF) [1, 5]. Etiopathogenetic mechanisms include metabolic and vascular factors, converging to oxidative stress and development of segmentary demyelinization and axonal (Waller) degeneration of the peripheral nerves of diabetic patients [2, 3]. The diabetic neuropathy (DN) is a “silent” pathology making the tissues of the feet very sensitive [1, 3, 5]. The neuropathic diabetic foot, as the heaviest complication of the DPNP, is a very frequent cause of amputation of the lower extremities in diabetic patients [1].
For the improvement of quality of life of patients with clinical patterns of the mentioned continuum is obligatory the composition of a complex rehabilitation programme, respecting the basic principles of synergism between active agents, including: strict glycemic control, medication (rheologically active drugs, peripheral vasodilatators, antioxidants, vitamins of B group); physiotherapy (exercises, soft tissue techniques, massages); preformed physical modalities (electric currents, magnetic fields; light, laser); self control of patients (hypoglucidic diet, daily physical activity, feet care) [1, 2, 3, 4, 5].
2.OBJECTIVE
The purpose of our study was to prove the significance of physical and rehabilitation medicine in the resolution of the practical problem diabetic polyneuropathy (DPNP) and diabetic foot (DF) and to evaluate quantitatively the effect on signs and symptoms of these patients of a complex physical therapeutic programme, including lasertherapy, physiotherapy and ergotherapy.
3.DESIGN OF THE STUDY
3.1.Material and methods:
The subjects of the study are 132 DPNP-patients (sensorimotor form, distal symmetric type) with developed diabetic foot (DF), divided in control and experimental groups. Patients were randomized to two treatment groups of 66 each one.
The rehabilitation programme includes in both groups: physiotherapy (analytic exercises, massage elements and mobilizations of the lower limbs) and patient education. In the experimental group we added too lasertherapy and ergotherapeutic activities.
The observed group comprised 64 males and 68 females, mean age 54 years (42-65); with type 2 DM at mean duration 7,3 years (7-17); treated with oral medication (stable in the last 3 months) and hypoglucid diet. Duration of DPNP was 4,8 years (from 12 months to 9 years). All patients had: sensory signs — acroparesthesias, dysesthesias, sensation of burning or cold feet, pain (evaluated with Visual analogue scale VAS 0-20); distal hypopallesthesia (measured with the vibroesthesiometer of Riedel-Seyfert 0-8, normal value 6-8); changes of the pression sense (measured by the 10 g monofilament of Semmes-Weinstein; altered thermosensibility (measured by tubes with cold or hot water); absent ankle jerks; motor weakness (peroneal paralysis in 72 patients; peroneal and tibial paralysis in 42 patients; peroneal, tibial and femoral paralysis in 18 patients). The Classical Electrodiagnostics (ED) of the lower limb nerves of the patients demonstrated quantitative and qualitative alterations of the excitability of the sensory and motor nerve fibers to galvanic and neofaradic currents (to partial reaction of degeneration /RD/ grade III); including changes in many parameters: reobasis, chronaxie, I/t curves, cutaneous electroresistance. In our patients we observed electromyographic (EMG) signs of segmental demyelinisation and axonal degeneration of the sensory and motor fibers of the peripheral nerves (diminished sensory and motor conduction velocity; increased latency and diminished amplitude of the M-response in stimulative EMG; missing of SNAP of the sural nerve) [3, 5]. In a lot of patients we observed microcirculatory acral disturbances and trophic alterations (distally in lower limbs), all patients had neuropathic diabetic foot of Charcot type — grade І and ІІ according to Shenaq classification [1, 5]. In laser-doppler-flowmetry we distinguished paradoxal sympathetic axon-reflex veno-arteriolar reactivity, diminished thermo-regulatory vasomotor response and reduced microvascular dilatatory capacity [5, 11].
We excluded from the observed group patients with general contra-indications for physical therapy; with co-morbidity – grave coronary insufficiency, evident radicular syndrome, significant ulcerations (diabetic foot grade III or more according to Shenaq classification); changes in the medication for the DM in the last two months before our investigation.
Patients were assessed for signs and symptoms of DM, DPNP and DF before and after treatment and one month later, according to the PROTOCOL including the history of disease and nosometric criteria of DM, DPNP and DF (patients’ complaints; clinical signs and symptoms – somatic, neurological, functional examination; assessment of pain and vibration sense; manual muscular testing; ED; EMG; laser-doppler-flowmetry; lab exams) [Koleva I. 1998-2005].
3.2.Ethic aspects
The investigation was conducted with consideration for the protection of patients, as outlined in the Declaration of Helsinki, and was approved by the appropriate institutional review board and ethic commission. All patients gave written informed consent before undergoing any examination or study procedure.
3.3.Physical and Rehabilitation Medicine (PRM) programme
In all patients the PRM programme includes physiotherapy = kinesitherapy according Bulgarian nomenclature {analytic exercises, massage elements and mobilizations of the lower limbs (active-assisted and active-resisted muscle strengthening exercises, 30 min., XV procedures)}. In all cases we applied too methods of patient education and a hypoglucid and hypolipid diet (number ІХ according to Pevzner’s list).
In the experimental group (group 2) we applied too preformed modalities (lasertherapy — standard dosage for amelioration of the tissue trophy, 3 min. for every foot, XV procedures)} and occupational therapy methods (designated to training activities of daily living, some of them – oriented to a professional qualification and re-orientation of diabetics).
3.4.Statistical analysis was performed with SPSS electronic package, version 11.5. We applied options for two samples comparison) with parametrical analysis of variances ANOVA and non-parametrical distribution (Wilcoxon signed rank test). The treatment difference was considered to be statistically significant if the p value was < 0.05. In some cases we received lower results of the p-value (p<0.01).
4.RESULTS AND ANALYSIS
The comparative analysis of results of exams and measures before (B.Th.) and after therapy (A.Th.) demonstrates a statistically significant beneficial effect (p<0,001) of our complex physical therapeutic and rehabilitation programme on some signs and symptoms (part of them remain stabilized one month after the end of the treatment): reduction of irritative sensory signs (Visual analogue scale — VAS, fig.1), enhance of hypopallesthesia (vibroesthesiometer of Riedel-Seifert, fig.2), increase of diminished pression sense (monofilament of Semmes-Weinstein, fig.3) and thermo perception (fig.4); tendency to normalization of quantitatively and qualitatively altered electro-excitability of peripheral nerves in response to stimulation with galvanic or neofaradic currents (results of classical electrodiagnostics, fig.5). We observed a tendency to increase of muscle strength of paretic muscles, but without statistical significance between both groups (results of manual muscular testing).
It is important to note the stability of effect one month after the end of physical therapy (the patient continues the prescribed exercise programme).
The most important (for diabetic patients) effect of the treatment was the reduction of irritative sensory signs – pain relief in lower extremities. Only in patients of the experimental group (with lasertherapy) we observed statistically significant (p<0,001) reduction of acroparesthesias, dysesthesias, sensation of burning or cold feet and pain (visualized by the analysis of Visual analogue scale VAS 0-20) (fig.1).
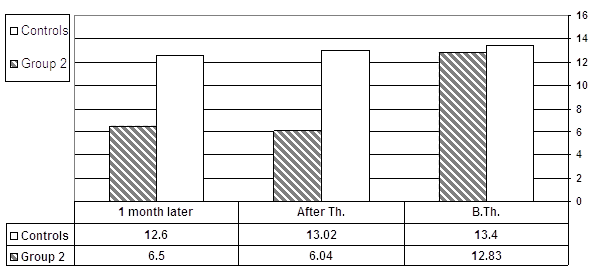
Fig.1. Pain relief (VAS 0-20)
Another favorable effect of the lasertherapy was the reduction of distally diminished vibratory sensibility, pression and thermo perception — objective criteria for qualitative and quantitative evaluation of the treatment efficacy. In all cases of the experimental group we observed statistically significant (p<0,001) increase of the distal hypopallesthesia (measured by vibroesthesiometer of Riedel-Seyfert for quantitative evaluation of the vibratory sensibility 0-8, normal values 6-8) (fig. 2); ofthe pression sense (10 g monofilament of Semmes-Weinstein 5.07 mm) (fig. 3) and of the thermo-sensibility (hot-cold) (fig. 4). No statistical significance in the control group.
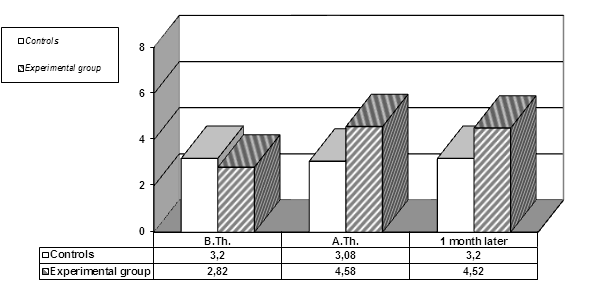
Fig.2. Amelioration of the hypopallesthesia (vibroesthesiometer of Riedel-Seyfert 0-8) —
B.Th., A.Th., one month later
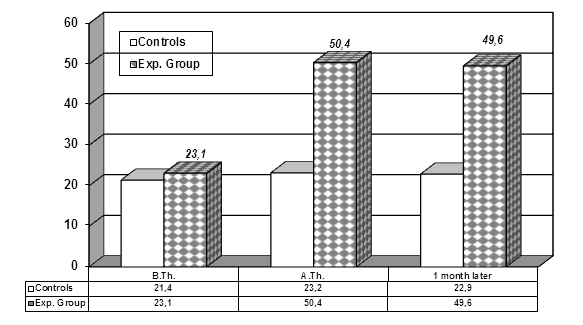
Fig.3. Dynamics in pression sense (10 g monofilament of Semmes-Weinstein 5.07mm)

Fig.4. Changes in thermo-sensibility
We observed significant improvement of the indicators of nerve electroexcitability using electroneurography — classical electrodiagnostic (ED) methods (fig.5). The estimated medians in Wilcoxon statistics are dynamic. The curve of distribution of patients (Gaus-distribution) A.Th. is transferred to the levels of minor alteration in comparison with the curve B.Th. The results of ED visualize the favorable effect of physical modalities on nerve and muscle excitability and reactions.
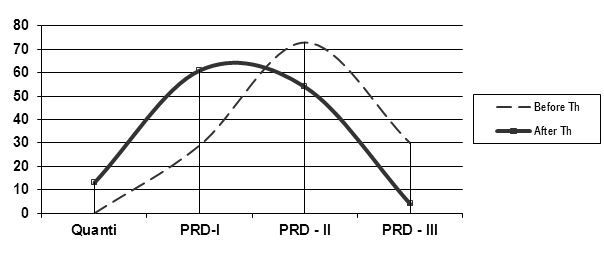
Fig.5. Distribution of the electrodiagnostic group (before and after therapy)-
quantitative alterations (Quanti), partial reaction of degeneration /PRD/ — levels I, II, III
The results of the manual muscular testing (ММТ) showed a tendency to increase of muscle strength of paretic muscles (but without statistical significance).
5.DISCUSSION
It’s proved that some pre-formed modalities (e.g. laser) provoque local vasodilatation, stimulate the metabolism and throphics of the tissues; help the regeneration of peripheral nerves and ameliorate the nerve irritability and conductivity [5, 6, 7, 8 , 9, 10]. In case of synergic combination between physical modalities the efficacy of physical therapy and rehabilitation is increasing.
The hypoesthesia, hypopallesthesia, disturbances of thermoperception, vegetovasal and vegetotrophic alterations in lower extremities of diabetics are improved significantly by laser. The peripheral motor weakness is favorably influenced by physiotherapy and occupational therapy activities – evaluated by manual muscle testing and classical electrodiagnostics (some of parameters without statistical significance for a 20-days course). It’s important to remind that for every diabetic patient even the simply delay of the progression of DPNP and DF is considered as a success. Most resistant to treatment are the “old” and “heaviest” paralyses, localized distally — in the extensors of the toes (especially m.extensor hallucis).
Our results proved that the complex rehabilitation ameliorates quality of life of diabetic patients. The complex PRM programme of care is able to recover consequences of neuronal dysfunctions, positive and negative neuropathic symptoms and pain. This is not only a symptomatic treatment, but also a pathogenetically oriented therapy and may delay, stop or even reverse the progression of the clinical continuum: metabolic syndrome -> NIDDM -> DPNP -> DF.
6.CONCLUSION
We could recommend our complex rehabilitation programme for treatment of the neuropathic DF. Intermittent courses of PRM programmes of care may be a successful adjuvant to drug treatment of DM, DPNP and DF. The development of the disease of these patients can be slowed down by organized and systematic physical therapy in specialized hospitals, combined with adequate medication, everyday physical activity and a strict glycemic control.
In our opinion the observation of diabetics should be done by a multi-disciplinary team (doctors — specialists in physical and rehabilitation medicine, in endocrinology and in neurology, specialists in dietology and physiotherapy, bachelors of kinesitherapy and medical rehabilitation and ergotherapy); following the scheme: clinic of neurology -> clinic of neurorehabilitation -> balneotherapeutic center -> rehabilitation service in the regional therapeutic center.
REFERENCES
- American Podiatric Medical Association. 1997 diabetes survey: statistical results. J Am Podiatr Med Assoc;1997;87(12):575-583.
- Apfel C., Kessler J.A., Adornato B.T., Litchy W.J., Sanders C., Rask C.A., and the NGF Study Group. Recombinant human nerve growth factor in the treatment of diabetic polyneuropathy. Neurology;1998;51:695-702.
- Echeverry D., Sherman A., Diabetic Neuropathy. E-Medicine Journal,2001;2:12.
- Fletcher G., Balady G., Amsterdam E., Exercise standards for testing and training: a statement for health professionals from the American Heart Association. Circulation; 2001;104(14):1694-1704.
- Koleva I.B., Contemporaneous possibilities of rehabilitation in diabetic neuropathy and diabetic foot. Monograph. Sofia: B.Stamenov, 2005. P.148. (In Bulgarian)
- Koleva I.B., Peripheral paralyses – changing the weakness management paradigm (pharmacological or non-pharmacological intervention – from disconnection to combination). Neurorehabilitation;2008;2(1):12-8.
- Koleva I.B., Impact of physical modalities in prevention and rehabilitation of diabetic polyneuropathy and neuropathic diabetic foot. – In: Diabetic Medications 2015: International Conference on Targeting Diabetes and Novel Therapeutics, Sept 2015 / U.S.A, Las Vegas, NV. Available at:
- Koleva I.B., Dikova M., Ioshinov R.D., Lishev N.S., Quantitative evaluation of efficacy of some physical therapeutic complexes on irritative sensory signs of diabetic polyneuropathy. European Journal of Neurology;2004;11 Suppl.2: S36-182.
- Koleva I.B., Iochinov R.D., Dikova M., Physical Therapy and Rehabilitation in Diabetic Polyneuropathy Patients. In: WJ Peek & GJ Lankhorst Editors. Physical and Rehabilitation MEDIMOND: Monduzzi Editore; 2001. p.677-681.
- Koleva I.B., Iochinov R.D., Stoyneva Z.B., Dikova M., Ontcheva G., Transcutaneous electroneurostimulation and fangotherapy in Diabetic Polyneuropathy Patients. Abstracts Book of the 3rd World Congress in Neurological Rehabilitation, Venice, April 2002: 497.
- Stoyneva B., Koleva I.B., Assessment of the physical therapy effect on diabetic distal autonomic and microcirculatory dysfunction by Laser Doppler flowmetry. Diabetes, Stoffwechsel und Herz; 2008;17:24-25.[schema type=»book» name=»SIGNIFICANCE OF LASERTHERAPY AND ERGOTHERAPY IN THE REHABILITATION OF NEUROPATHIC DIABETIC FOOT» description=»The purpose of our study is to prove the significance of physical and rehabilitation medicine to the practical problem diabetic polyneuropathy (DPNP) and diabetic foot (DF) and to evaluate quantitatively the effect on signs and symptoms of these patients of a complex physical therapeutic programme, including lasertherapy, physiotherapy and ergotherapy. Material and methods: The subjects of the study are 132 DPNP-patients (sensorimotor form, distal symmetric type) with developed diabetic foot (DF), divided in control and experimental groups. The rehabilitation programme includes in both groups: physiotherapy (analytic exercises, massage elements and mobilizations of the lower limbs) and patient education. In the experimental group we added too lasertherapy and ergotherapeutic activities. For database management we used t-test (analysis of variances ANOVA) and Wilcoxon signed rank test (non-parametric distribution analysis). The comparative analysis of results before and after therapy demonstrates a statistically significant beneficial effect of the complex programme in the experimental group on some signs and symptoms (part of them remain stabilized one month after treatment): irritative sensory signs (VAS), hypopallesthesia (vibroesthesiometer of Riedel-Seifert), pression sense (monofilament of Semmes-Weinstein), thermosensibility; altered electroexcitability and conductibility of peripheral nerves and muscles (excitomotory electrodiagnostics); vegetovasal and vegetotrophic disturbances (Shenaq evaluation). No significant effect on the muscle strength of the paretic muscles (manual muscular testing). Conclusion: The complex rehabilitation ameliorates quality of life of diabetic patients.» author=»Koleva Ivet B., Yoshinov Radoslav D.» publisher=»БАСАРАНОВИЧ ЕКАТЕРИНА» pubdate=»2017-01-09″ edition=»euroasia-science.ru_29-30.12.2015_12(21)» ebook=»yes» ]